Research on Ethics, Aging, and Community Health, Medford, Massachusetts.
Departments of Occupational Therapy and Community Health, Tufts University, Medford, Massachusetts.
J Am Soc Nephrol. 2021 Jun 1;32(6):1527-1535. doi: 10.1681/ASN.2020091298. Epub 2021 Apr 7.
Older patients with advanced CKD are at high risk for serious complications and death, yet few discuss advance care planning (ACP) with their kidney clinicians. Examining barriers and facilitators to ACP among such patients might help identify patient-centered opportunities for improvement.
In semistructured interviews in March through August 2019 with purposively sampled patients (aged ≥70 years, CKD stages 4-5, nondialysis), care partners, and clinicians at clinics in across the United States, participants described discussions, factors contributing to ACP completion or avoidance, and perceived value of ACP. We used thematic analysis to analyze data.
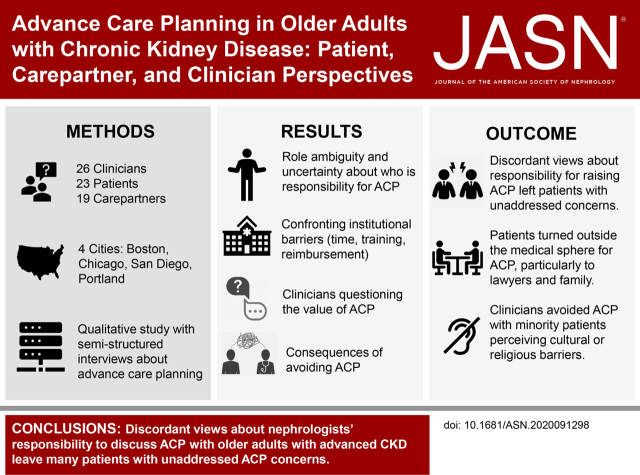
We conducted 68 semistructured interviews with 23 patients, 19 care partners, and 26 clinicians. Only seven of 26 (27%) clinicians routinely discussed ACP. About half of the patients had documented ACP, mostly outside the health care system. We found divergent ACP definitions and perspectives; kidney clinicians largely defined ACP as completion of formal documentation, whereas patients viewed it more holistically, wanting discussions about goals, prognosis, and disease trajectory. Clinicians avoided ACP with patients from minority groups, perceiving cultural or religious barriers. Four themes and subthemes informing variation in decisions to discuss ACP and approaches emerged: () role ambiguity and responsibility for ACP, () questioning the value of ACP, () confronting institutional barriers (time, training, reimbursement, and the electronic medical record, EMR), and () consequences of avoiding ACP (disparities in ACP access and overconfidence that patients' wishes are known).
Patients, care partners, and clinicians hold discordant views about the responsibility for discussing ACP and the scope for it. This presents critical barriers to the process, leaving ACP insufficiently discussed with older adults with advanced CKD.
患有晚期 CKD 的老年患者有发生严重并发症和死亡的高风险,但他们很少与肾脏临床医生讨论预先医疗护理计划(ACP)。研究此类患者进行 ACP 的障碍和促进因素,可能有助于确定以患者为中心的改进机会。
2019 年 3 月至 8 月,我们在美国各地的诊所通过半结构式访谈,对有目的抽样的患者(年龄≥70 岁,CKD 分期 4-5 期,非透析)、护理伙伴和临床医生进行访谈,参与者描述了讨论、促成 ACP 完成或避免的因素,以及对 ACP 的感知价值。我们使用主题分析对数据进行分析。
我们共进行了 68 次半结构式访谈,受访者包括 23 名患者、19 名护理伙伴和 26 名临床医生。26 名临床医生中只有 7 名(27%)常规讨论 ACP。约一半的患者有记录在案的 ACP,大多是在医疗体系之外。我们发现 ACP 的定义和观点存在差异;肾脏临床医生主要将 ACP 定义为完成正式文件,但患者更全面地看待 ACP,希望讨论目标、预后和疾病轨迹。临床医生避免与少数族裔患者讨论 ACP,认为存在文化或宗教障碍。有四个主题和子主题可以解释讨论 ACP 和方法的差异:(1)ACP 角色的模糊性和责任、(2)对 ACP 价值的质疑、(3)应对机构障碍(时间、培训、报销和电子病历(EMR))以及(4)避免 ACP 的后果(ACP 机会不均等和过度自信地认为患者的意愿是已知的)。
患者、护理伙伴和临床医生对讨论 ACP 的责任和范围持有不同的看法。这对这一过程构成了重大障碍,导致老年 CKD 患者的 ACP 讨论不足。