Mukerji Shibani S, Das Sudeshna, Alabsi Haitham, Brenner Laura N, Jain Aayushee, Magdamo Colin, Collens Sarah I, Ye Elissa, Keller Kiana, Boutros Christine L, Leone Michael J, Newhouse Amy, Foy Brody, Li Matthew D, Lang Min, Anahtar Melis N, Shao Yu-Ping, Ge Wendong, Sun Haoqi, Triant Virginia A, Kalpathy-Cramer Jayashree, Higgins John, Rosand Jonathan, Robbins Gregory K, Westover M Brandon
Department of Neurology, Massachusetts General Hospital, Boston, MA, United States.
Harvard Medical School, Boston, MA, United States.
Front Neurol. 2021 Apr 9;12:642912. doi: 10.3389/fneur.2021.642912. eCollection 2021.
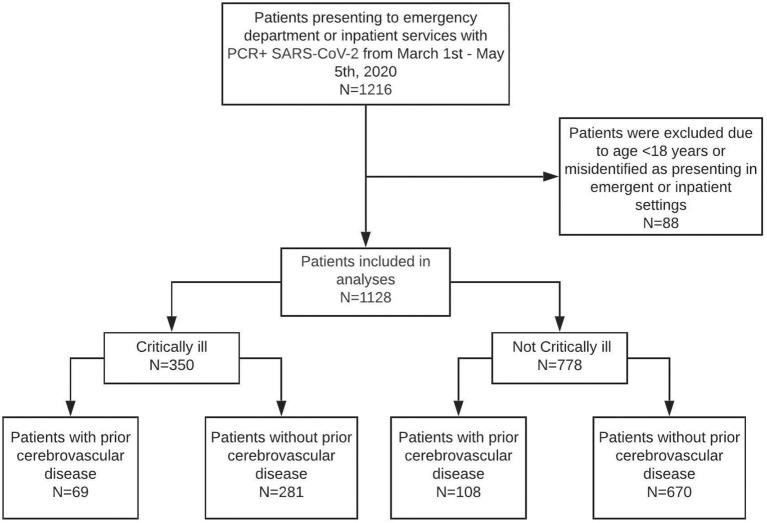
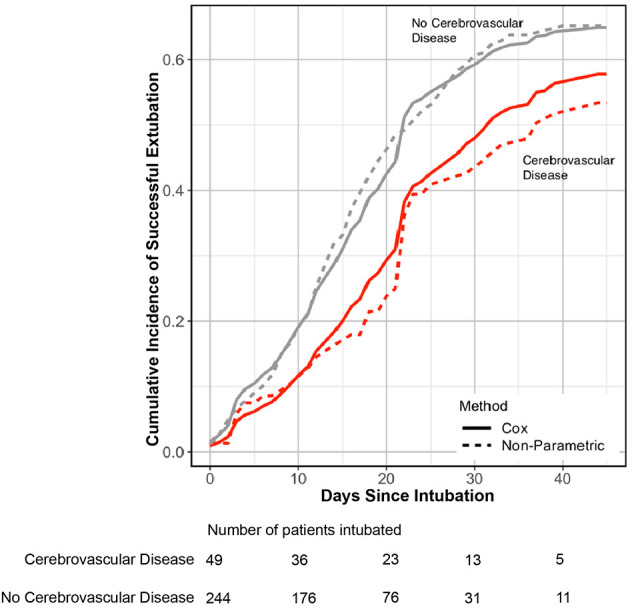
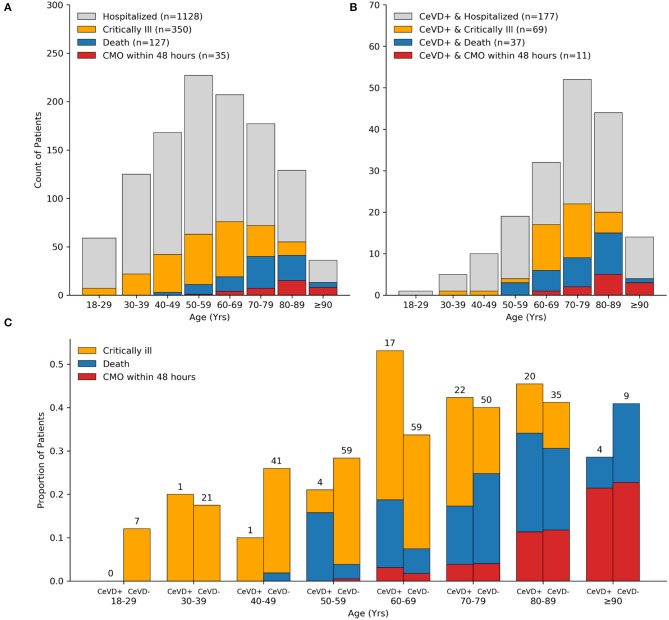
Patients with comorbidities are at increased risk for poor outcomes in COVID-19, yet data on patients with prior neurological disease remains limited. Our objective was to determine the odds of critical illness and duration of mechanical ventilation in patients with prior cerebrovascular disease and COVID-19. A observational study of 1,128 consecutive adult patients admitted to an academic center in Boston, Massachusetts, and diagnosed with laboratory-confirmed COVID-19. We tested the association between prior cerebrovascular disease and critical illness, defined as mechanical ventilation (MV) or death by day 28, using logistic regression with inverse probability weighting of the propensity score. Among intubated patients, we estimated the cumulative incidence of successful extubation without death over 45 days using competing risk analysis. Of the 1,128 adults with COVID-19, 350 (36%) were critically ill by day 28. The median age of patients was 59 years (SD: 18 years) and 640 (57%) were men. As of June 2nd, 2020, 127 (11%) patients had died. A total of 177 patients (16%) had a prior cerebrovascular disease. Prior cerebrovascular disease was significantly associated with critical illness (OR = 1.54, 95% CI = 1.14-2.07), lower rate of successful extubation (cause-specific HR = 0.57, 95% CI = 0.33-0.98), and increased duration of intubation (restricted mean time difference = 4.02 days, 95% CI = 0.34-10.92) compared to patients without cerebrovascular disease. Prior cerebrovascular disease adversely affects COVID-19 outcomes in hospitalized patients. Further study is required to determine if this subpopulation requires closer monitoring for disease progression during COVID-19.
患有合并症的患者在新冠病毒病(COVID-19)中出现不良结局的风险增加,但关于既往有神经疾病患者的数据仍然有限。我们的目标是确定既往有脑血管疾病且感染COVID-19的患者发生危重症的几率以及机械通气的持续时间。对连续收治于马萨诸塞州波士顿一家学术中心并经实验室确诊为COVID-19的1128例成年患者进行了一项观察性研究。我们使用倾向评分的逆概率加权逻辑回归,测试了既往脑血管疾病与危重症之间的关联,危重症定义为在第28天进行机械通气(MV)或死亡。在插管患者中,我们使用竞争风险分析估计了45天内无死亡成功拔管的累积发生率。在1128例COVID-19成年患者中,350例(36%)在第28天时病情危重。患者的中位年龄为59岁(标准差:18岁),640例(57%)为男性。截至2020年6月2日,127例(11%)患者死亡。共有177例患者(16%)既往有脑血管疾病。与无脑血管疾病的患者相比,既往脑血管疾病与危重症显著相关(比值比=1.54,95%置信区间=1.14-2.07),成功拔管率较低(病因特异性风险比=0.57,95%置信区间=0.33-0.98),插管持续时间延长(受限平均时间差=4.02天,95%置信区间=0.34-10.92)。既往脑血管疾病对住院患者的COVID-19结局有不利影响。需要进一步研究以确定该亚组患者在COVID-19期间是否需要更密切地监测疾病进展。