Yamamoto Ryo, Sasaki Junichi, Shibusawa Takayuki, Nakada Taka-Aki, Mayumi Toshihiko, Takasu Osamu, Matsuda Kenichi, Shimazui Takashi, Otsubo Hiroki, Teshima Yuto, Nabeta Masakazu, Moriguchi Takeshi, Oda Shigeto
Department of Emergency and Critical Care Medicine, Keio University School of Medicine, Tokyo, Japan.
Department of Emergency and Critical Care Medicine, Chiba University Graduate School of Medicine, Chiba, Japan.
Crit Care Explor. 2021 Apr 26;3(4):e0387. doi: 10.1097/CCE.0000000000000387. eCollection 2021 Apr.
Several inflammation markers have been reported to be associated with unfavorable clinical outcomes in critically ill patients. We aimed to elucidate whether serum interleukin-6 concentration considered with Sequential Organ Failure Assessment score can better predict mortality in critically ill patients.
A prospective observational study.
Five university hospitals in 2016-2018.
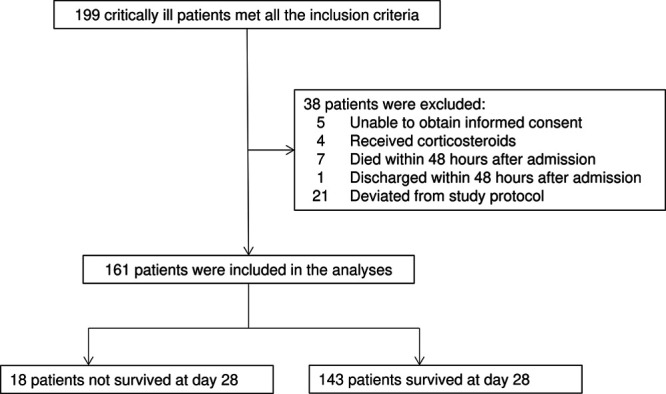
Critically ill adult patients who met greater than or equal to two systemic inflammatory response syndrome criteria at admission were included, and those who died or were discharged within 48 hours were excluded.
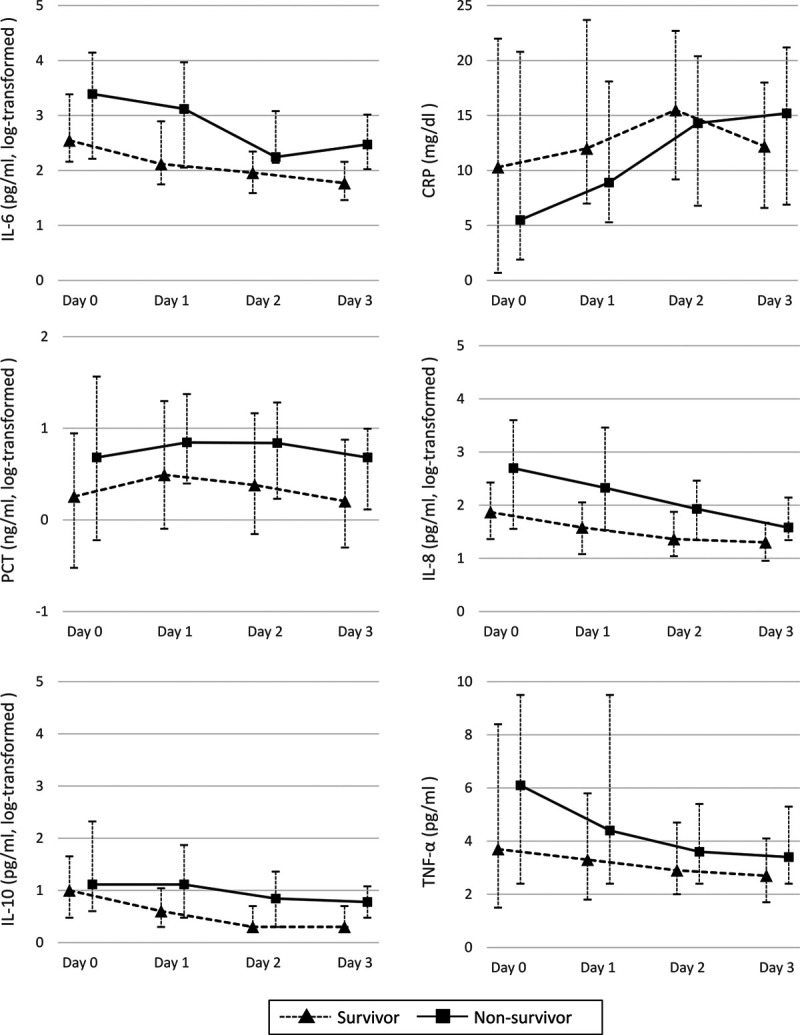
Inflammatory biomarkers including interleukin (interleukin)-6, -8, and -10; tumor necrosis factor-α; C-reactive protein; and procalcitonin were blindly measured daily for 3 days. Area under the receiver operating characteristic curve for Sequential Organ Failure Assessment score at day 2 according to 28-day mortality was calculated as baseline. Combination models of Sequential Organ Failure Assessment score and additional biomarkers were developed using logistic regression, and area under the receiver operating characteristic curve calculated in each model was compared with the baseline.
Among 161 patients included in the study, 18 (11.2%) did not survive at day 28. Univariate analysis for each biomarker identified that the interleukin-6 (days 1-3), interleukin-8 (days 0-3), and interleukin-10 (days 1-3) were higher in nonsurvivors than in survivors. Analyses of 28-day mortality prediction by a single biomarker showed interleukin-6, -8, and -10 at days 1-3 had a significant discrimination power, and the interleukin-6 at day 3 had the highest area under the receiver operating characteristic curve (0.766 [0.656-0.876]). The baseline area under the receiver operating characteristic curve for Sequential Organ Failure Assessment score predicting 28-day mortality was 0.776 (0.672-0.880). The combination model using additional interleukin-6 at day 3 had higher area under the receiver operating characteristic curve than baseline (area under the receiver operating characteristic curve = 0.844, area under the receiver operating characteristic curve improvement = 0.068 [0.002-0.133]), whereas other biomarkers did not improve accuracy in predicting 28-day mortality.
Accuracy for 28-day mortality prediction was improved by adding serum interleukin-6 concentration to Sequential Organ Failure Assessment score.
有报道称,几种炎症标志物与危重症患者不良临床结局相关。我们旨在阐明,将血清白细胞介素-6浓度与序贯器官衰竭评估(SOFA)评分相结合,是否能更好地预测危重症患者的死亡率。
一项前瞻性观察性研究。
2016年至2018年期间的五所大学医院。
纳入入院时符合大于或等于两条全身炎症反应综合征标准的成年危重症患者,排除入院48小时内死亡或出院的患者。
连续3天每天对炎症生物标志物进行盲测,包括白细胞介素(IL)-6、-8、-10、肿瘤坏死因子-α、C反应蛋白和降钙素原。计算根据第28天死亡率得出的第2天SOFA评分的受试者工作特征曲线下面积作为基线。使用逻辑回归建立SOFA评分与其他生物标志物的联合模型,并将每个模型计算出的受试者工作特征曲线下面积与基线进行比较。
本研究纳入的161例患者中,18例(11.2%)在第28天未存活。对每种生物标志物的单因素分析发现,非存活者的白细胞介素-6(第1 - 3天)、白细胞介素-8(第0 - 3天)和白细胞介素-10(第1 - 3天)水平高于存活者。单一生物标志物对28天死亡率预测的分析显示,第1 - 3天的白细胞介素-6、-8和-10具有显著的辨别能力,第3天的白细胞介素-6的受试者工作特征曲线下面积最高(0.766[0.656 - 0.876])。预测28天死亡率的SOFA评分的基线受试者工作特征曲线下面积为0.776(0.672 - 0.880)。第3天额外加入白细胞介素-6的联合模型的受试者工作特征曲线下面积高于基线(受试者工作特征曲线下面积 = 0.844,受试者工作特征曲线下面积改善 = 0.068[0.002 - 0.133]),而其他生物标志物并未提高预测28天死亡率的准确性。
在SOFA评分中加入血清白细胞介素-6浓度可提高28天死亡率预测的准确性。