Department of Biomedical Sciences, Jockey Club College of Veterinary Medicine and Life Sciences, City University of Hong Kong, Hong Kong, China.
Department of Infection Biology, Faculty of Infectious and Tropical Diseases, London School of Hygiene & Tropical Medicine, London, UK.
BMC Infect Dis. 2021 May 5;21(1):424. doi: 10.1186/s12879-021-06115-6.
Although by late February 2020 the COVID-19 epidemic was effectively controlled in Wuhan, China, estimating the effects of interventions, such as transportation restrictions and quarantine measures, on the early COVID-19 transmission dynamics in Wuhan is critical for guiding future virus containment strategies. Since the exact number of infected cases is unknown, the number of documented cases was used by many disease transmission models to infer epidemiological parameters. This means that it was possible to produce biased estimates of epidemiological parameters and hence of the effects of intervention measures, because the percentage of all cases that were documented changed during the first 2 months of the epidemic, as a consequence of a gradually improving diagnostic capability.
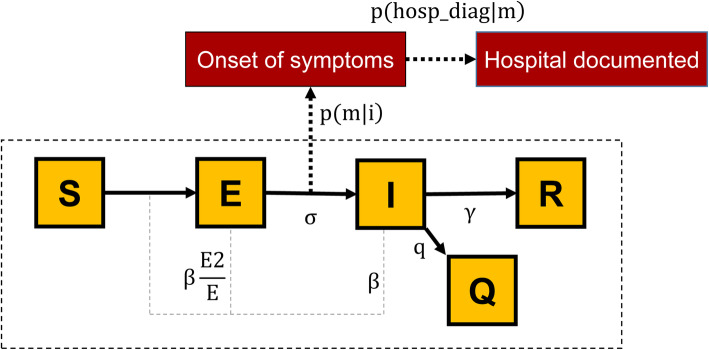
To overcome these limitations, we constructed a stochastic susceptible-exposed-infected-quarantined-recovered (SEIQR) model, accounting for intervention measures and temporal changes in the proportion of new documented infections out of total new infections, to characterize the transmission dynamics of COVID-19 in Wuhan across different stages of the outbreak. Pre-symptomatic transmission was taken into account in our model, and all epidemiological parameters were estimated using the Particle Markov-chain Monte Carlo (PMCMC) method.
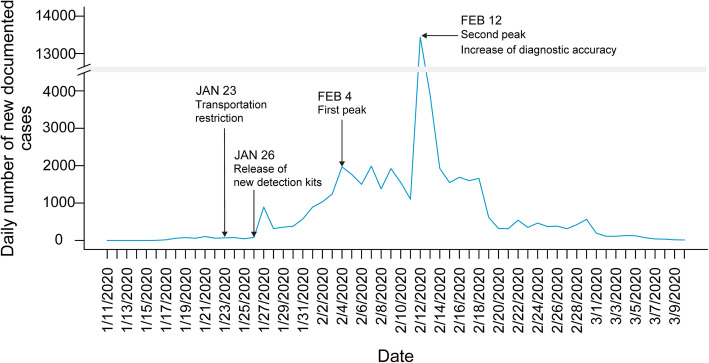
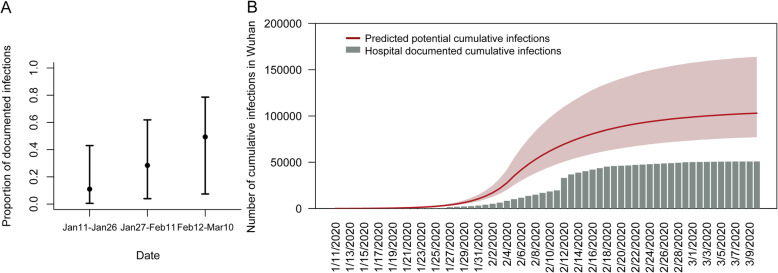
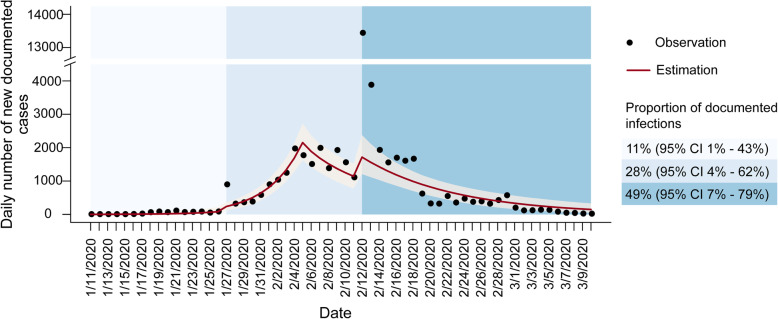
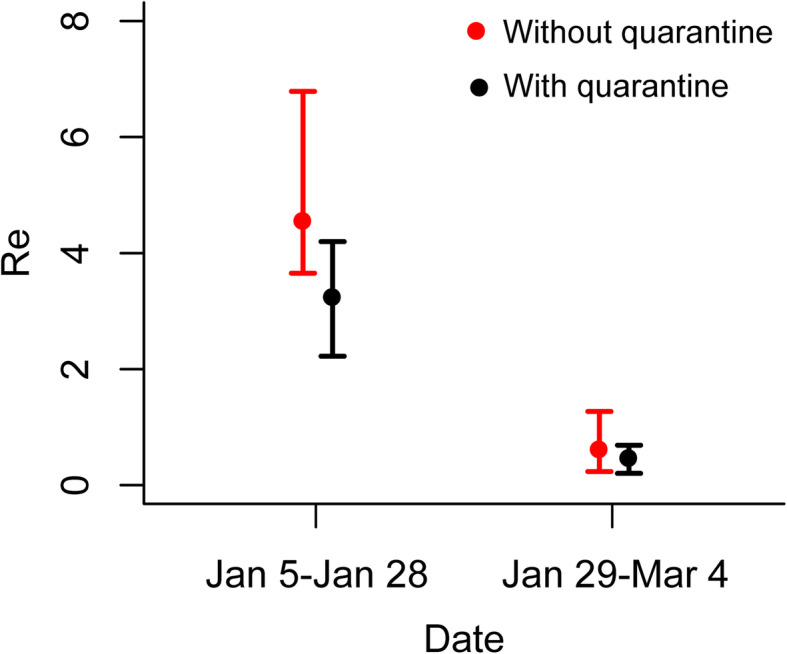
Our model captured the local Wuhan epidemic pattern as two-peak transmission dynamics, with one peak on February 4 and the other on February 12, 2020. The impact of intervention measures determined the timing of the first peak, leading to an 86% drop in the R from 3.23 (95% CI, 2.22 to 4.20) to 0.45 (95% CI, 0.20 to 0.69). The improved diagnostic capability led to the second peak and a higher proportion of documented infections. Our estimated proportion of new documented infections out of the total new infections increased from 11% (95% CI 1-43%) to 28% (95% CI 4-62%) after January 26 when more detection kits were released. After the introduction of a new diagnostic criterion (case definition) on February 12, a higher proportion of daily infected cases were documented (49% (95% CI 7-79%)).
Transportation restrictions and quarantine measures together in Wuhan were able to contain local epidemic growth.
尽管到 2020 年 2 月下旬,中国武汉的 COVID-19 疫情已得到有效控制,但评估交通限制和检疫措施等干预措施对武汉 COVID-19 早期传播动态的影响,对于指导未来的病毒遏制策略至关重要。由于确切的感染人数未知,因此许多疾病传播模型都使用已记录的病例数来推断流行病学参数。这意味着,由于诊断能力逐渐提高,在疫情的头 2 个月中,所有病例中记录在案的病例比例发生了变化,因此有可能对流行病学参数产生有偏差的估计,从而对干预措施的效果产生偏差。
为了克服这些限制,我们构建了一个随机的易感-暴露-感染-隔离-恢复(SEIQR)模型,该模型考虑了干预措施以及新记录感染病例在总新感染病例中的比例随时间的变化,以描述 COVID-19 在武汉不同阶段的传播动态。我们的模型考虑了症状前传播,所有流行病学参数均使用粒子马尔可夫链蒙特卡罗(PMCMC)方法进行估计。
我们的模型捕捉到了武汉当地的疫情模式,即双峰传播动力学,第一个高峰出现在 2020 年 2 月 4 日,第二个高峰出现在 2 月 12 日。干预措施的影响决定了第一个高峰的时间,导致 R 从 3.23(95%置信区间,2.22 至 4.20)下降到 0.45(95%置信区间,0.20 至 0.69),降幅为 86%。诊断能力的提高导致了第二个高峰和更高比例的记录感染病例。我们估计的新记录感染病例在总新感染病例中的比例从 1 月 26 日(当更多的检测试剂盒发布时)的 11%(95%置信区间 1-43%)增加到 28%(95%置信区间 4-62%)。在 2 月 12 日引入新的诊断标准(病例定义)后,更多的每日感染病例被记录(49%(95%置信区间 7-79%))。
武汉的交通限制和检疫措施共同成功遏制了当地疫情的增长。