Division of Cardiology, Department of Medicine, Massachusetts General Hospital, 55 Fruit Street, GRB 8, Boston, MA, 02114, USA.
Cardiovascular Disease Initiative, Broad Institute of Harvard University and the Massachusetts Institute of Technology, Cambridge, MA, USA.
Eur Heart J. 2021 Jul 1;42(25):2472-2483. doi: 10.1093/eurheartj/ehab250.
Physical activity may be an important modifiable risk factor for atrial fibrillation (AF), but associations have been variable and generally based on self-reported activity.
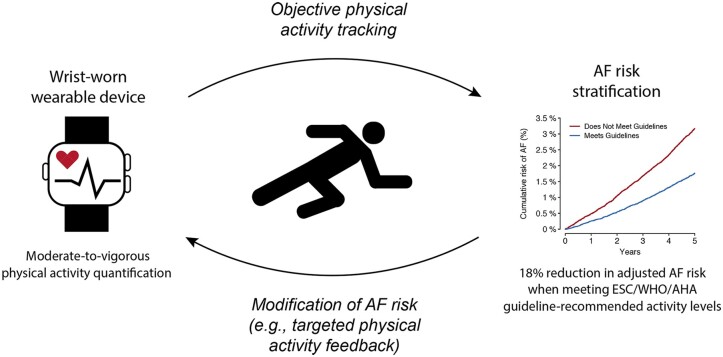
We analysed 93 669 participants of the UK Biobank prospective cohort study without prevalent AF who wore a wrist-based accelerometer for 1 week. We categorized whether measured activity met the standard recommendations of the European Society of Cardiology, American Heart Association, and World Health Organization [moderate-to-vigorous physical activity (MVPA) ≥150 min/week]. We tested associations between guideline-adherent activity and incident AF (primary) and stroke (secondary) using Cox proportional hazards models adjusted for age, sex, and each component of the Cohorts for Heart and Aging Research in Genomic Epidemiology AF (CHARGE-AF) risk score. We also assessed correlation between accelerometer-derived and self-reported activity. The mean age was 62 ± 8 years and 57% were women. Over a median of 5.2 years, 2338 incident AF events occurred. In multivariable adjusted models, guideline-adherent activity was associated with lower risks of AF [hazard ratio (HR) 0.82, 95% confidence interval (CI) 0.75-0.89; incidence 3.5/1000 person-years, 95% CI 3.3-3.8 vs. 6.5/1000 person-years, 95% CI 6.1-6.8] and stroke (HR 0.76, 95% CI 0.64-0.90; incidence 1.0/1000 person-years, 95% CI 0.9-1.1 vs. 1.8/1000 person-years, 95% CI 1.6-2.0). Correlation between accelerometer-derived and self-reported MVPA was weak (Spearman r = 0.16, 95% CI 0.16-0.17). Self-reported activity was not associated with incident AF or stroke.
Greater accelerometer-derived physical activity is associated with lower risks of AF and stroke. Future preventive efforts to reduce AF risk may be most effective when targeting adherence to objective activity thresholds.
体力活动可能是心房颤动(AF)的一个重要可改变的风险因素,但相关性一直存在差异,且通常基于自我报告的活动。
我们分析了英国生物库前瞻性队列研究中 93669 名无先前存在的 AF 且佩戴腕部加速度计进行 1 周的参与者。我们将测量活动是否符合欧洲心脏病学会、美国心脏协会和世界卫生组织的标准建议进行分类[中等到剧烈体力活动(MVPA)≥150 分钟/周]。我们使用 Cox 比例风险模型测试了与指南一致的活动与事件性 AF(主要)和中风(次要)之间的关联,该模型调整了年龄、性别和基因组流行病学中心脏与衰老研究队列(CHARGE-AF)风险评分的每个组成部分。我们还评估了加速度计衍生和自我报告活动之间的相关性。平均年龄为 62±8 岁,57%为女性。在中位数为 5.2 年的随访期间,发生了 2338 例事件性 AF。在多变量调整模型中,与指南一致的活动与 AF 风险降低相关[风险比(HR)0.82,95%置信区间(CI)0.75-0.89;发病率 3.5/1000 人年,95%CI 3.3-3.8 与 6.5/1000 人年,95%CI 6.1-6.8]和中风(HR 0.76,95%CI 0.64-0.90;发病率 1.0/1000 人年,95%CI 0.9-1.1 与 1.8/1000 人年,95%CI 1.6-2.0)。加速度计衍生和自我报告的 MVPA 之间的相关性较弱(Spearman r=0.16,95%CI 0.16-0.17)。自我报告的活动与事件性 AF 或中风无关。
加速度计衍生的体力活动越多,AF 和中风的风险越低。未来预防 AF 风险的努力可能最有效,当针对目标活动阈值的依从性时。