Centre for Global Infectious Disease Analysis, School of Public Health, Imperial College London.
Department of Non-communicable Disease Epidemiology, London School of Hygiene and Tropical Medicine, London, United Kingdom.
Eur J Cancer. 2021 Jul;152:233-242. doi: 10.1016/j.ejca.2021.04.019. Epub 2021 May 5.
Delays in cancer diagnosis arose from the commencement of non-pharmaceutical interventions (NPI) introduced in the UK in March 2020 in response to the COVID-19 pandemic. Our earlier work predicted this will lead to approximately 3620 avoidable deaths for four major tumour types (breast, bowel, lung, and oesophageal cancer) in the next 5 years. Here, using national population-based modelling, we estimate the health and economic losses resulting from these avoidable cancer deaths. We also compare these with the impact of an equivalent number of COVID-19 deaths to understand the welfare consequences of the different health conditions.
We estimate health losses using quality-adjusted life years (QALYs) and lost economic productivity using the human capital (HC) approach. The analysis uses linked English National Health Service (NHS) cancer registration and hospital administrative datasets for patients aged 15-84 years, diagnosed with breast, colorectal, and oesophageal cancer between 1st Jan to 31st Dec 2010, with follow-up data until 31st Dec 2014, and diagnosed with lung cancer between 1st Jan to 31st Dec 31 2012, with follow-up data until 31st Dec 2015. Productivity losses are based on the estimation of excess additional deaths due to cancer at 1, 3 and 5 years for the four cancer types, which were derived from a previous analysis using this dataset. A total of 500 random samples drawn from the total number of COVID-19 deaths reported by the Office for National Statistics, stratified by gender, were used to estimate productivity losses for an equivalent number of deaths (n = 3620) due to SARS-CoV-2 infection.
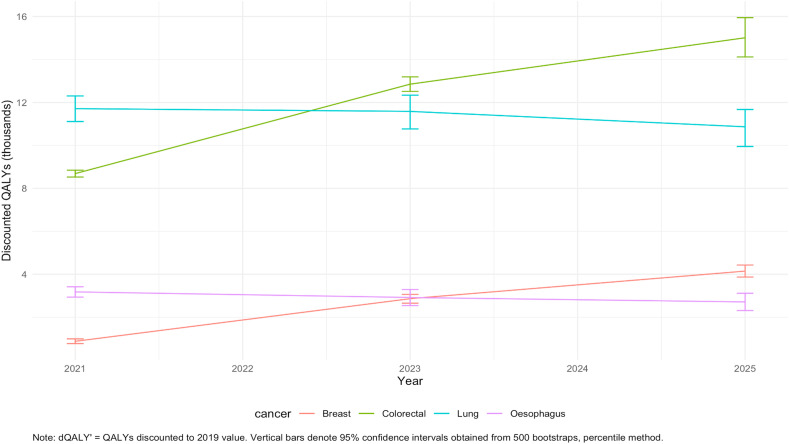
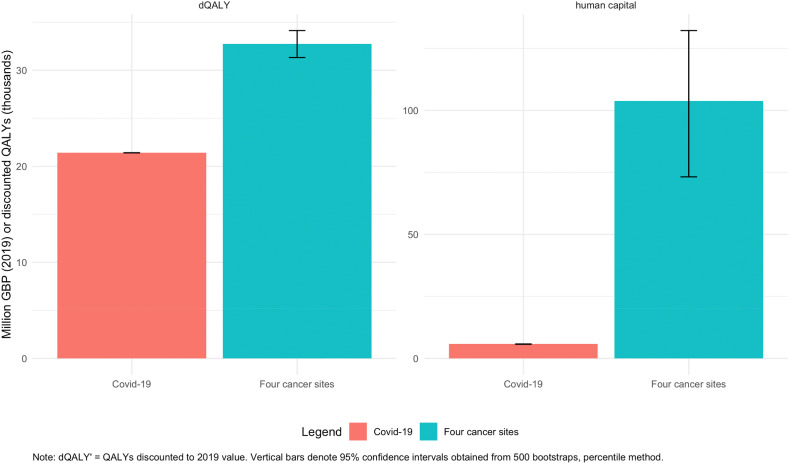
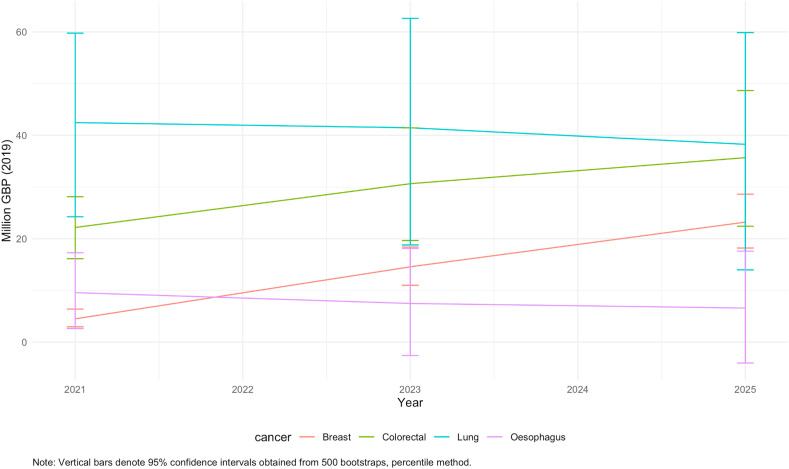
We collected data for 32,583 patients with breast cancer, 24,975 with colorectal cancer, 6744 with oesophageal cancer, and 29,305 with lung cancer. We estimate that across the four site-specific cancers combined in England alone, additional excess cancer deaths would amount to a loss of 32,700 QALYs (95% CI 31,300-34,100) and productivity losses of £103.8million GBP (73.2-132.2) in the next five years. For breast cancer, we estimate a loss of 4100 QALYS (3900-4400) and productivity losses of £23.2 m (18.2-28.6); for colorectal cancer, 15,000 QALYS (14,100-16,000) lost and productivity losses of £35.7 m (22.4-48.7); for lung cancer 10,900 QALYS (9,900-11,700) lost and productivity losses of £38.3 m (14.0-59.9) for lung cancer; and for oesophageal cancer, 2700 QALYS (2300-3,100) lost and productivity losses of £6.6 m (-6 to -17.6). In comparison, the equivalent number of COVID-19 deaths caused approximately 21,450 QALYs lost, as well as productivity losses amounting to £76.4 m (73.5-79.2).
Premature cancer deaths resulting from diagnostic delays during the first wave of the COVID-19 pandemic in the UK will result in significant economic losses. On a per-capita basis, this impact is, in fact, greater than that of deaths directly attributable to COVID-19. These results emphasise the importance of robust evaluation of the trade-offs of the wider health, welfare and economic effects of NPI to support both resource allocation and the prioritisation of time-critical health services directly impacted in a pandemic, such as cancer care.
由于 2020 年 3 月英国为应对 COVID-19 大流行而开始实施非药物干预(NPI),癌症诊断出现了延误。我们之前的研究预测,在未来 5 年内,这将导致四种主要肿瘤类型(乳腺癌、结直肠癌、肺癌和食管癌)中约有 3620 人可避免死亡。在这里,我们使用全国人群建模来估计这些可避免的癌症死亡造成的健康和经济损失。我们还将这些损失与同等数量的 COVID-19 死亡进行了比较,以了解不同健康状况的福利后果。
我们使用质量调整生命年(QALYs)来估计健康损失,并使用人力资本(HC)方法来估计经济生产力损失。该分析使用链接的英国国家卫生服务(NHS)癌症登记和医院管理数据集,用于 2010 年 1 月 1 日至 12 月 31 日期间诊断为乳腺癌、结直肠癌和食管癌的年龄在 15-84 岁之间的患者,随访数据截至 2014 年 12 月 31 日,以及 2012 年 1 月 1 日至 12 月 31 日诊断为肺癌的患者,随访数据截至 2015 年 12 月 31 日。生产力损失基于对四种癌症类型中由于癌症而导致的额外死亡人数的估计,这些额外死亡人数是从使用该数据集的先前分析中得出的。从国家统计局报告的 COVID-19 死亡总数中随机抽取了 500 个样本,按性别分层,用于估计由于 SARS-CoV-2 感染而导致的同等数量的死亡(n=3620)的生产力损失。
我们收集了 32583 名乳腺癌患者、24975 名结直肠癌患者、6744 名食管癌患者和 29305 名肺癌患者的数据。我们估计,仅在英格兰,这四种特定部位癌症的总和将导致额外的癌症死亡人数增加 32700 个 QALYs(95%CI 31300-34100),生产力损失为 10380 万英镑(7320-13220 万英镑)在接下来的五年中。对于乳腺癌,我们估计损失 4100 个 QALYs(3900-4400)和 2320 万英镑的生产力损失(1820-2860 万英镑); 对于结直肠癌,损失 15000 个 QALYs(14100-16000)和 3570 万英镑的生产力损失(2240-4870 万英镑); 对于肺癌,损失 10900 个 QALYs(9900-11700)和 3830 万英镑的生产力损失(1400-5990 万英镑); 对于食管癌,损失 2700 个 QALYs(2300-3100)和 660 万英镑的生产力损失(-6 至-17.6)。相比之下,同等数量的 COVID-19 死亡导致约 21450 个 QALYs 丧失,以及 7640 万英镑的生产力损失(735-792 万英镑)。
英国 COVID-19 大流行第一波期间诊断延误导致的癌症死亡将导致重大经济损失。按人均计算,这种影响实际上大于直接归因于 COVID-19 的死亡。这些结果强调了对更广泛的健康、福利和经济影响进行稳健评估的重要性,以支持资源分配和优先考虑直接受大流行影响的时间关键型卫生服务,如癌症护理。