Infectious Diseases Unit, Hospital General Universitario de Elche, Alicante, Spain; Clinical Medicine Department, Universidad Miguel Hernández, Alicante, Spain.
Infectious Diseases Unit, Hospital General Universitario de Elche, Alicante, Spain.
J Autoimmun. 2021 Sep;123:102703. doi: 10.1016/j.jaut.2021.102703. Epub 2021 Jul 20.
Durability of the humoral immune response to SARS-CoV-2 has yet to be defined. We longitudinally evaluated during a 12-month period the antibody responses to SARS-CoV-2, and analysed predictors of antibody titres decline and seroreversion.
Prospective study conducted in a cohort of patients hospitalized for microbiologically-confirmed COVID-19. Blood and nasopharyngeal samples were sequentially obtained during hospital stay and at 1, 2, 6 and 12 months after patients' discharge for measuring anti-spike (S) and anti-nucleocapsid (N) IgG antibody levels and SARS-CoV-2 RNA, respectively.
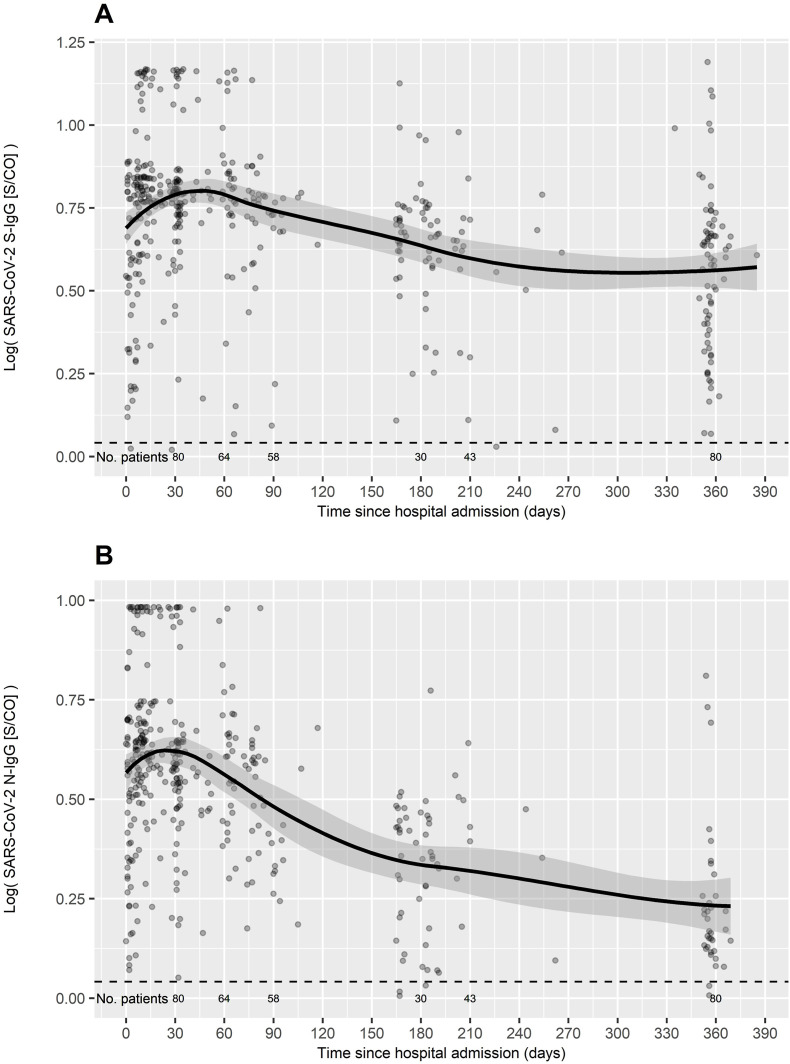
80 non-vaccinated patients were analysed. At month 12 after discharge, 73 (91.2%) patients exhibited detectable S-IgG and 35 (43.8%) N-IgG antibody titres. A gradual wane was observed in S-IgG and N-IgG antibody titres. Linear regression showed that S-IgG decline was positively associated with peak antibody titres (coefficient [95% CI] 0.059 [0.05-0.067], p < 0.001), inversely with WHO severity score (coefficient [95% CI] -0.042 [-0.079/-0.004], p = 0.033), and there was a trivial positive association with age (coefficient [95% CI] 0.002 [0-0.005], p = 0.10); N-IgG decline was positively associated with peak antibody titres (coefficient [95% CI] 0.091 [0.078-0.105], p < 0.001). Logistic regression showed that seroreversion for S-IgG was inversely associated with peak S-IgG (OR 0.19; 95% CI, 0.04-0.45; p = 0.004); seroreversion for N-IgG was inversely associated with peak N-IgG (OR 0.71; 95% 0.53-0.90; p = 0.009) and positively with cycle threshold of RT-PCR (OR 1.14; 95% CI, 1.00-1.33; p = 0.062).
Anti-spike IgG antibodies remain detectable one year after hospitalization for COVID-19. Higher peak antibody titres and disease severity were associated with increased durability of detectable antibodies.
SARS-CoV-2 的体液免疫反应的持久性尚未确定。我们在 12 个月的时间内对 SARS-CoV-2 的抗体反应进行了纵向评估,并分析了抗体滴度下降和血清学转换的预测因素。
这是一项前瞻性研究,纳入了因微生物学确诊的 COVID-19 住院的患者队列。在患者出院后 1、2、6 和 12 个月,分别通过测量抗刺突(S)和抗核衣壳(N)IgG 抗体水平和 SARS-CoV-2 RNA ,对住院期间和出院后采集的血液和鼻咽样本进行了连续检测。
分析了 80 名未接种疫苗的患者。出院后 12 个月时,73 例(91.2%)患者可检测到 S-IgG,35 例(43.8%)患者可检测到 N-IgG 抗体滴度。S-IgG 和 N-IgG 抗体滴度逐渐下降。线性回归显示,S-IgG 下降与峰值抗体滴度呈正相关(系数[95%CI]0.059[0.05-0.067],p<0.001),与世界卫生组织严重程度评分呈负相关(系数[95%CI]-0.042[-0.079/-0.004],p=0.033),与年龄呈轻微正相关(系数[95%CI]0.002[0-0.005],p=0.10);N-IgG 下降与峰值抗体滴度呈正相关(系数[95%CI]0.091[0.078-0.105],p<0.001)。Logistic 回归显示,S-IgG 血清学转换与峰值 S-IgG 呈负相关(OR 0.19;95%CI,0.04-0.45;p=0.004);N-IgG 血清学转换与峰值 N-IgG 呈负相关(OR 0.71;95%CI,0.53-0.90;p=0.009),与 RT-PCR 的循环阈值呈正相关(OR 1.14;95%CI,1.00-1.33;p=0.062)。
COVID-19 住院患者出院后一年仍可检测到抗刺突 IgG 抗体。较高的峰值抗体滴度和疾病严重程度与可检测抗体的持久性增加有关。