Batterham Philip J, Calear Alison L, Sunderland Matthew, Kay-Lambkin Frances, Farrer Louise M, Christensen Helen, Gulliver Amelia
Centre for Mental Health Research, Research School of Population Health, The Australian National University, Canberra, Australia.
The Matilda Centre for Research in Mental Health and Substance Use, University of Sydney, Sydney, Australia.
J Med Internet Res. 2021 Jul 27;23(7):e23029. doi: 10.2196/23029.
Psychosocial, self-guided, internet-based programs are effective in treating depression and anxiety. However, the community uptake of these programs is poor. Recent approaches to increasing engagement (defined as both uptake and adherence) in internet-based programs include brief engagement facilitation interventions (EFIs). However, these programs require evaluation to assess their efficacy.
The aims of this hybrid implementation effectiveness trial are to examine the effects of a brief internet-based EFI presented before an internet-based cognitive behavioral therapy self-help program (myCompass 2) in improving engagement (uptake and adherence) with that program (primary aim), assess the relative efficacy of the myCompass 2 program, and determine whether greater engagement was associated with improved efficacy (greater reduction in depression or anxiety symptoms) relative to the control (secondary aim).
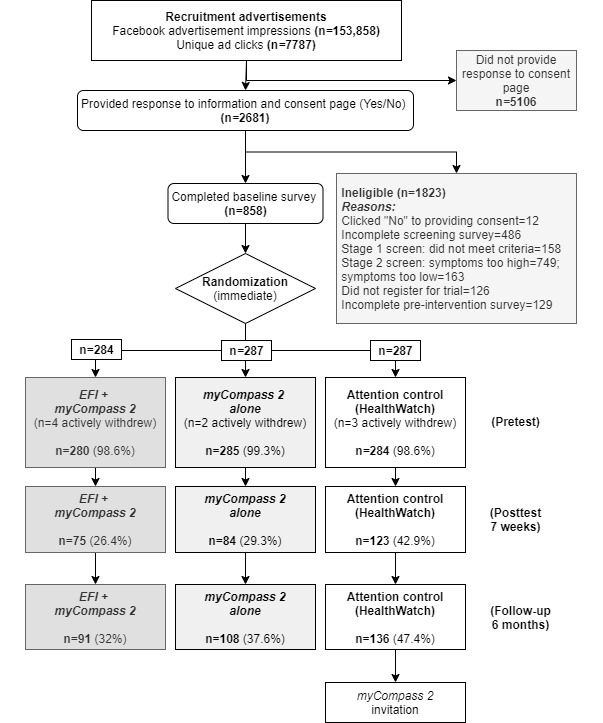
A 3-arm randomized controlled trial (N=849; recruited via social media) assessed the independent efficacy of the EFI and myCompass 2. The myCompass 2 program was delivered with or without the EFI; both conditions were compared with an attention control condition. The EFI comprised brief (5 minutes), tailored audio-visual content on a series of click-through linear webpages.
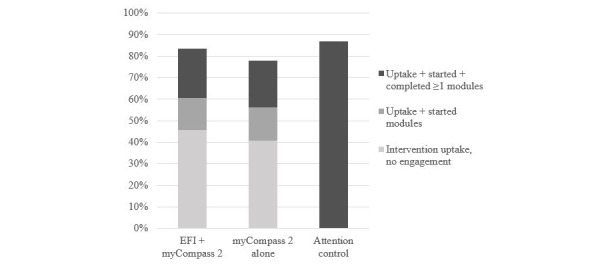
Uptake was high in all groups; 82.8% (703/849) of participants clicked through the intervention following the pretest survey. However, the difference in uptake between the EFI + myCompass 2 condition (234/280, 83.6%) and the myCompass 2 alone condition (222/285, 77.9%) was not significant (n=565; χ=29.2; P=.09). In addition, there was no significant difference in the proportion of participants who started any number of modules (1-14 modules) versus those who started none between the EFI + myCompass 2 (214/565, 37.9%) and the myCompass 2 alone (210/565, 37.2%) conditions (n=565; χ<0.1; P=.87). Finally, there was no significant difference between the EFI + myCompass 2 and the myCompass 2 alone conditions in the number of modules started (U=39366.50; z=-0.32; P=.75) or completed (U=39494.0; z=-0.29; P=.77). The myCompass 2 program was not found to be efficacious over time for symptoms of depression (F=1.16; P=.33) or anxiety (F=0.12; P=.98). However, planned contrasts suggested that myCompass 2 may have been effective for participants with elevated generalized anxiety disorder symptoms (F=3.50; P=.01).
This brief internet-based EFI did not increase the uptake of or adherence to an existing internet-based program for depression and anxiety. Individuals' motivation to initiate and complete internet-based self-guided interventions is complex and remains a significant challenge for self-guided interventions.
Australian New Zealand Clinical Trials Registry ACTRN12618001565235; https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=375839.
社会心理、自我引导的基于互联网的项目在治疗抑郁症和焦虑症方面是有效的。然而,这些项目在社区中的接受度较低。最近提高基于互联网项目参与度(定义为接受度和依从性)的方法包括简短的参与促进干预(EFI)。然而,这些项目需要进行评估以评估其疗效。
这项混合实施效果试验的目的是检验在基于互联网的认知行为疗法自助项目(myCompass 2)之前呈现的简短基于互联网的EFI对提高该项目的参与度(接受度和依从性)的效果(主要目的),评估myCompass 2项目的相对疗效,并确定相对于对照组,更高的参与度是否与更好的疗效(抑郁或焦虑症状的更大减轻)相关(次要目的)。
一项三臂随机对照试验(N = 849;通过社交媒体招募)评估了EFI和myCompass 2的独立疗效。myCompass 2项目在有或没有EFI的情况下提供;将这两种情况与注意力控制组进行比较。EFI包括在一系列点击式线性网页上的简短(5分钟)、量身定制的视听内容。
所有组的接受度都很高;82.8%(703/849)的参与者在预测试调查后点击了干预内容。然而,EFI + myCompass 2组(234/280,83.6%)和仅myCompass 2组(222/285,77.9%)之间的接受度差异不显著(n = 565;χ = 29.2;P = 0.09)。此外,在开始任何数量模块(1 - 14个模块)的参与者比例与未开始任何模块的参与者比例之间,EFI + myCompass 2组(214/565,37.9%)和仅myCompass 2组(210/565,37.2%)之间没有显著差异(n = 565;χ < 0.1;P = 0.87)。最后,EFI + myCompass 2组和仅myCompass 2组在开始模块数量(U = 39366.50;z = -0.32;P = 0.75)或完成模块数量(U = 39494.0;z = -0.29;P = 0.77)方面没有显著差异。随着时间的推移,未发现myCompass 2项目对抑郁症状(F = 1.16;P = 0.33)或焦虑症状(F = 0.12;P = 0.98)有效。然而,计划对比表明,myCompass 2可能对广泛性焦虑症症状升高的参与者有效(F = 3.50;P = 0.01)。
这种简短的基于互联网的EFI并没有提高现有基于互联网的抑郁症和焦虑症项目的接受度或依从性。个人发起和完成基于互联网的自我引导干预的动机很复杂,仍然是自我引导干预面临的重大挑战。
澳大利亚新西兰临床试验注册中心ACTRN12618001565235;https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=375839。