Department of Epidemiology and Biostatistics, School of Public Health, Xi'an Jiaotong University Health Science Center, Xi'an, China.
National Cancer Center/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
JAMA Netw Open. 2021 Aug 2;4(8):e2121403. doi: 10.1001/jamanetworkopen.2021.21403.
Upper gastrointestinal tract cancer, including esophageal and gastric cancers, in China accounts for 50% of the global burden. Endoscopic screening may be associated with a decreased incidence of and mortality from upper gastrointestinal tract cancer.
To evaluate the cost-effectiveness of endoscopic screening for esophageal and gastric cancers among people aged 40 to 69 years in areas of China where the risk of these cancers is high.
DESIGN, SETTING, AND PARTICIPANTS: For this economic evaluation, a Markov model was constructed for initial screening at different ages from a health care system perspective, and 5 endoscopic screening strategies with different frequencies (once per lifetime and every 10 years, 5 years, 3 years, and 2 years) were evaluated. The study was conducted between January 1, 2019, and October 31, 2020. Model parameters were estimated based on this project, government documents, and published literature. For each initial screening age (40-44, 45-49, 50-54, 55-59, 60-64, and 65-69 years), a closed cohort of 100 000 participants was assumed to enter the model and follow the alternative strategies.
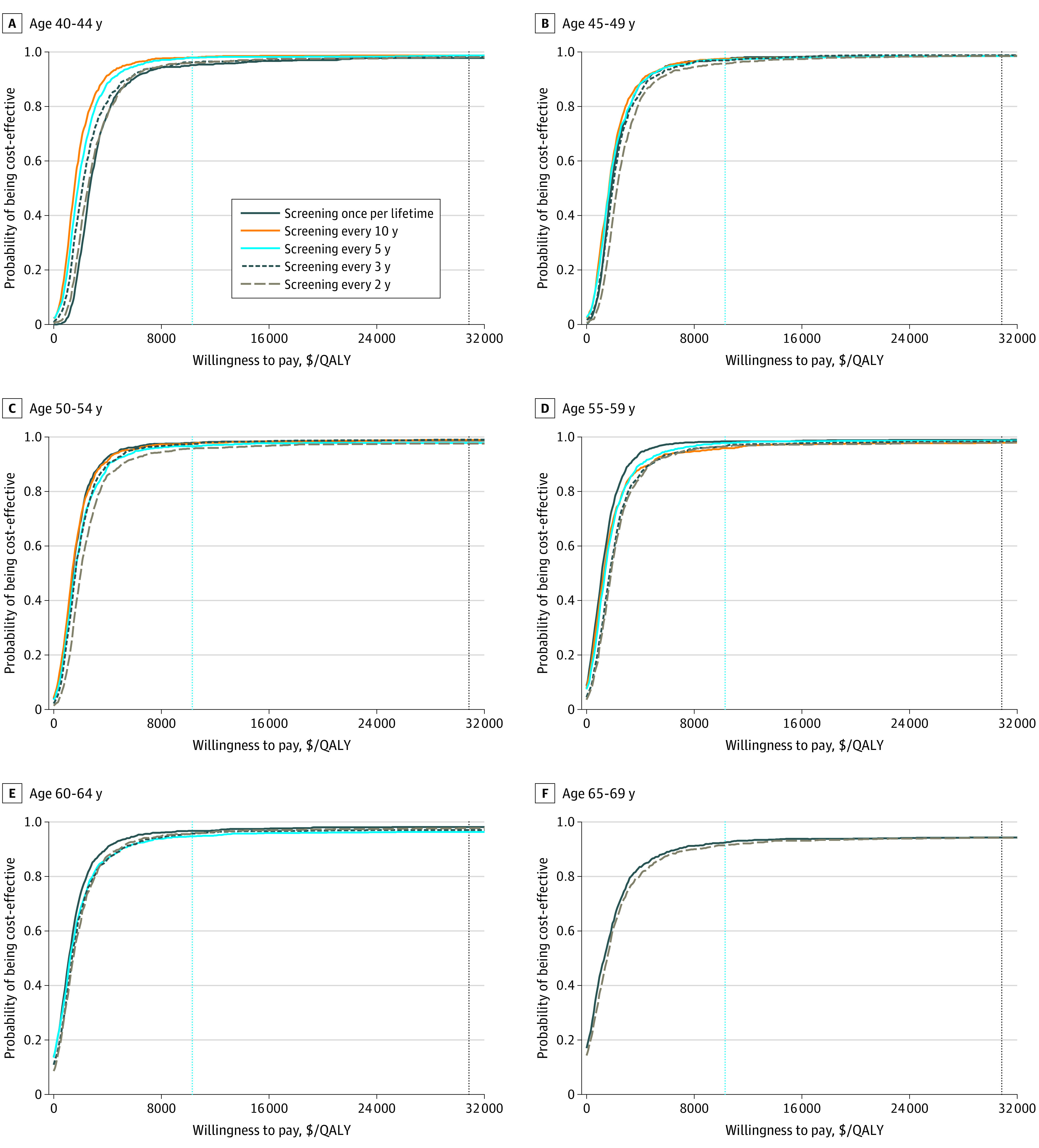
Cost-effectiveness was measured by calculating the incremental cost-effectiveness ratio (ICER), and the willingness-to-pay threshold was assumed to be 3 times the per capita gross domestic product in China (US $10 276). Univariate and probabilistic sensitivity analyses were conducted to assess the robustness of model findings.
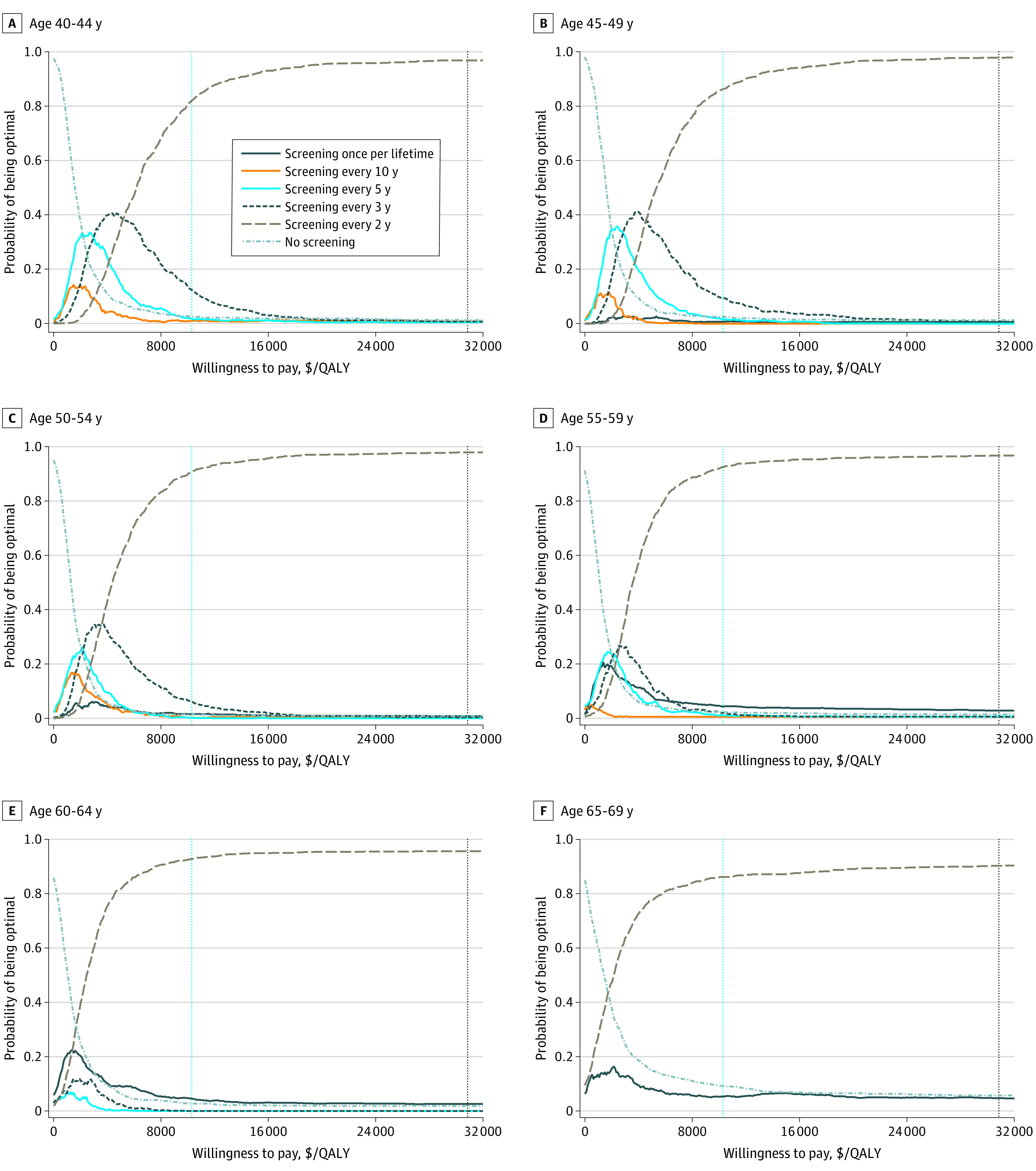
The study included a hypothetical cohort of 100 000 individuals aged 40 to 69 years. All 5 screening strategies were associated with improved effectiveness by 1087 to 10 362 quality-adjusted life-years (QALYs) and increased costs by US $3 299 000 to $22 826 000 compared with no screening over a lifetime, leading to ICERs of US $1343 to $3035 per QALY. Screening at a higher frequency was associated with an increase in QALYs and costs; ICERs for higher frequency screening compared with the next-lower frequency screening were between US $1087 and $4511 per QALY. Screening every 2 years would be the most cost-effective strategy, with probabilities of 90% to 98% at 3 times the per capita gross domestic product of China. The model was the most sensitive to utility scores of esophageal cancer- or gastric cancer-related health states and compliance with screening.
The findings suggest that combined endoscopic screening for esophageal and gastric cancers may be cost-effective in areas of China where the risk of these cancers is high; screening every 2 years would be the optimal strategy. These data may be useful for development of policies targeting the prevention and control of upper gastrointestinal tract cancer in China.
在中国,包括食管癌和胃癌在内的上消化道癌占全球负担的 50%。内镜筛查可能与上消化道癌的发病率和死亡率降低有关。
评估在中国上消化道癌风险较高的地区,40 至 69 岁人群进行食管和胃癌内镜筛查的成本效益。
设计、设置和参与者:本经济评估从卫生保健系统的角度出发,为初始筛查构建了一个 Markov 模型,并评估了 5 种不同频率(终生一次和每 10 年、5 年、3 年和 2 年)的内镜筛查策略。研究于 2019 年 1 月 1 日至 2020 年 10 月 31 日进行。模型参数基于该项目、政府文件和已发表的文献进行估计。对于每个初始筛查年龄(40-44 岁、45-49 岁、50-54 岁、55-59 岁、60-64 岁和 65-69 岁),假设一个 100000 人的封闭队列进入模型并遵循替代策略。
通过计算增量成本效益比(ICER)来衡量成本效益,假设中国人均国内生产总值的 3 倍(33090 美元)为意愿支付阈值。进行了单变量和概率敏感性分析,以评估模型结果的稳健性。
该研究纳入了一个假设的 100000 名 40 至 69 岁人群的队列。与终生不筛查相比,所有 5 种筛查策略均通过提高 1087 至 10362 个质量调整生命年(QALY)来提高效果,并增加 329.9 万至 2282.6 万美元的成本,导致每 QALY 的 ICER 为 1343 至 3035 美元。更高的筛查频率与 QALY 和成本的增加有关;与下一较低频率筛查相比,更高频率筛查的 ICER 为每 QALY 1087 至 4511 美元。每 2 年筛查一次将是最具成本效益的策略,在中国人均国内生产总值的 3 倍时,概率为 90%至 98%。该模型对食管癌或胃癌相关健康状况和筛查依从性的效用评分最为敏感。
研究结果表明,在中国上消化道癌风险较高的地区,联合进行食管和胃癌内镜筛查可能具有成本效益;每 2 年筛查一次将是最佳策略。这些数据可能有助于制定针对中国上消化道癌预防和控制的政策。