Department of Public Health and Primary Care, Katholieke Universiteit Leuven, Leuven, Belgium
Research Foundation Flanders, Brussel, Belgium.
BMJ Open. 2021 Aug 17;11(8):e047576. doi: 10.1136/bmjopen-2020-047576.
To describe the discrimination and calibration of clinical prediction models, identify characteristics that contribute to better predictions and investigate predictors that are associated with unplanned hospital readmissions.
Systematic review and meta-analysis.
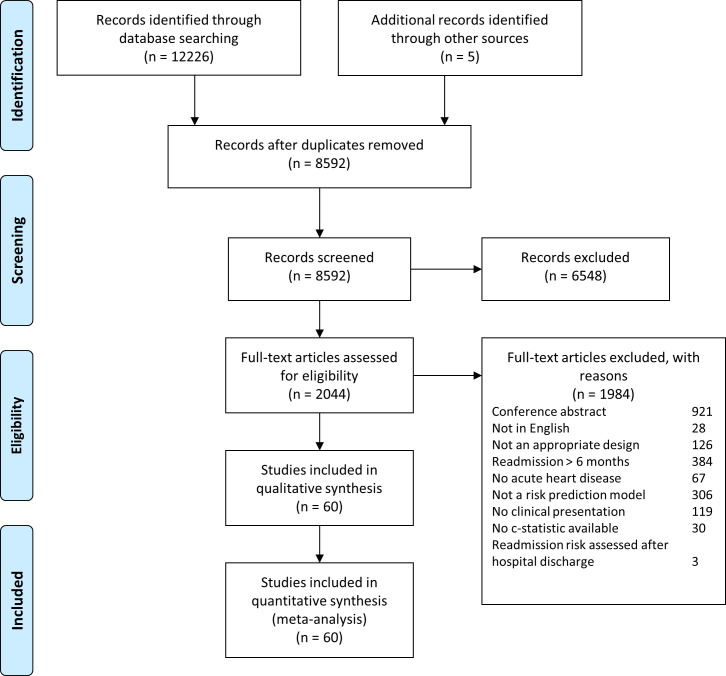
Medline, EMBASE, ICTPR (for study protocols) and Web of Science (for conference proceedings) were searched up to 25 August 2020.
Studies were eligible if they reported on (1) hospitalised adult patients with acute heart disease; (2) a clinical presentation of prediction models with c-statistic; (3) unplanned hospital readmission within 6 months.
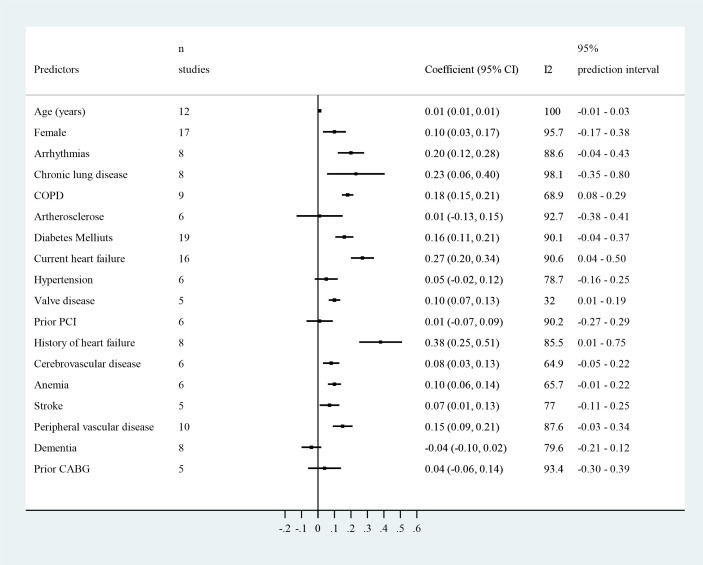
Model discrimination for unplanned hospital readmission within 6 months measured using concordance (c) statistics and model calibration. Meta-regression and subgroup analyses were performed to investigate predefined sources of heterogeneity. Outcome measures from models reported in multiple independent cohorts and similarly defined risk predictors were pooled.
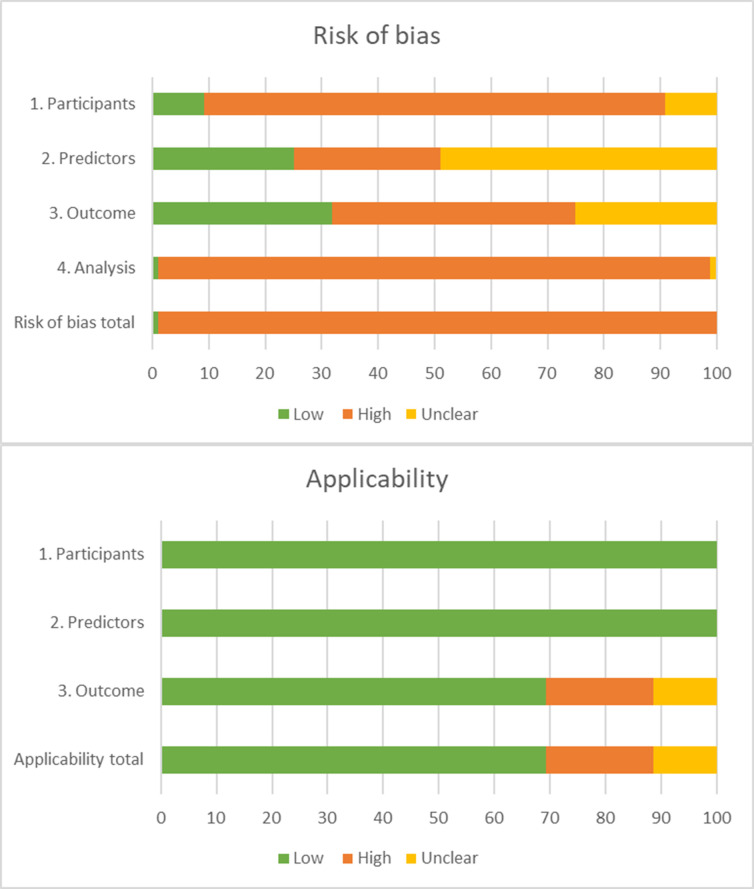
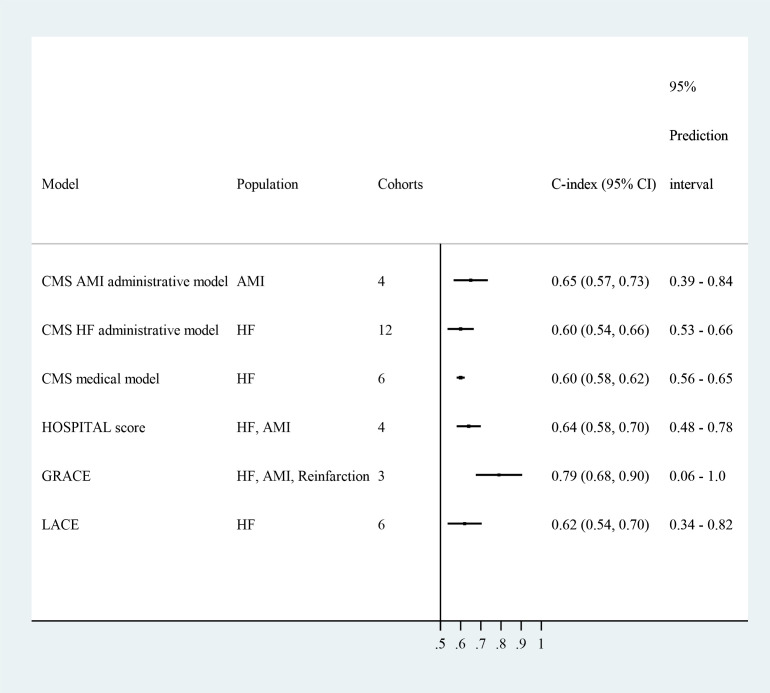
Sixty studies describing 81 models were included: 43 models were newly developed, and 38 were externally validated. Included populations were mainly patients with heart failure (HF) (n=29). The average age ranged between 56.5 and 84 years. The incidence of readmission ranged from 3% to 43%. Risk of bias (RoB) was high in almost all studies. The c-statistic was <0.7 in 72 models, between 0.7 and 0.8 in 16 models and >0.8 in 5 models. The study population, data source and number of predictors were significant moderators for the discrimination. Calibration was reported for 27 models. Only the GRACE (Global Registration of Acute Coronary Events) score had adequate discrimination in independent cohorts (0.78, 95% CI 0.63 to 0.86). Eighteen predictors were pooled.
Some promising models require updating and validation before use in clinical practice. The lack of independent validation studies, high RoB and low consistency in measured predictors limit their applicability.
CRD42020159839.
描述临床预测模型的区分度和校准度,确定有助于提高预测效果的特征,并研究与非计划性住院再入院相关的预测因素。
系统评价和荟萃分析。
截至 2020 年 8 月 25 日,检索了 Medline、EMBASE、ICTPR(用于研究方案)和 Web of Science(用于会议论文集)。
如果研究报告了(1)患有急性心脏疾病的住院成年患者;(2)预测模型的临床表现与 C 统计量;(3)6 个月内非计划性住院再入院,则符合纳入标准。
使用一致性(c)统计量测量 6 个月内非计划性住院再入院的模型区分度和模型校准度。进行了荟萃回归和亚组分析,以研究预定的异质性来源。从多个独立队列报告的模型和类似定义的风险预测因素中汇总了结果指标。
共纳入了 60 项描述 81 个模型的研究:43 个模型是新开发的,38 个是外部验证的。纳入的人群主要是心力衰竭(HF)患者(n=29)。平均年龄在 56.5 岁至 84 岁之间。再入院率从 3%到 43%不等。几乎所有研究的偏倚风险(RoB)都很高。72 个模型的 C 统计量<0.7,16 个模型的 C 统计量在 0.7 和 0.8 之间,5 个模型的 C 统计量>0.8。研究人群、数据来源和预测因素数量是区分度的显著调节因素。27 个模型报告了校准情况。只有 GRACE(全球急性冠状动脉事件注册)评分在独立队列中具有良好的区分度(0.78,95%CI 0.63 至 0.86)。汇总了 18 个预测因素。
一些有前途的模型需要更新和验证,然后才能在临床实践中使用。缺乏独立验证研究、高 RoB 和测量预测因素的一致性低限制了它们的适用性。
PROSPERO 注册号:CRD42020159839。