Krishnan Anand, Dar Lalit, Amarchand Ritvik, Prabhakaran Aslesh Ottapura, Kumar Rakesh, Rajkumar Prabu, Kanungo Suman, Bhardwaj Sumit Dutt, Choudekar Avinash, Potdar Varsha, Chakrabarti Alok Kumar, Kumar Cp Girish, Parameswaran Giridara Gopal, Dhakad Shivram, Manna Byomkesh, Choudhary Ashish, Lafond Kathryn E, Azziz-Baumgartner Eduardo, Saha Siddhartha
Centre for Community Medicine, All India Institute of Medical Sciences, New Delhi, India
Department of Microbiology, All India Institute of Medical Sciences, New Delhi, India.
BMJ Open. 2021 Oct 7;11(10):e052473. doi: 10.1136/bmjopen-2021-052473.
We describe here a multicentric community-dwelling cohort of older adults (60 years of age) established to estimate incidence, study risk factors, healthcare utilisation and economic burden associated with influenza and respiratory syncytial virus (RSV) in India.
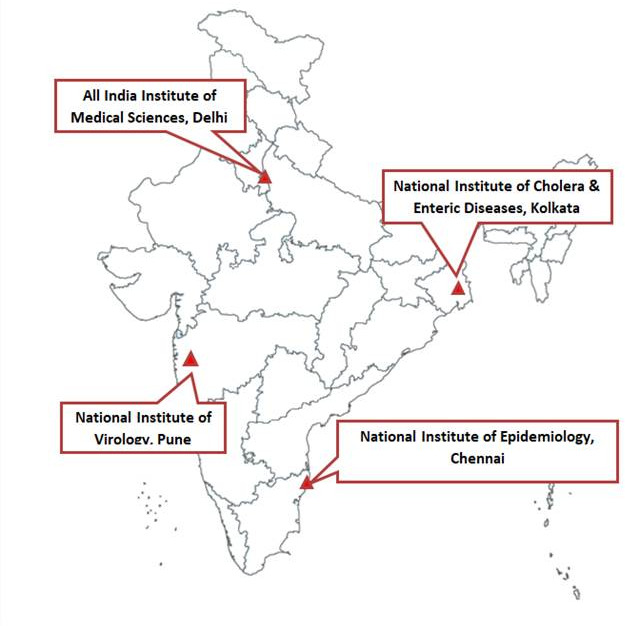
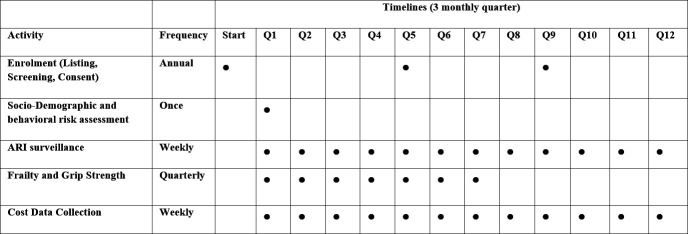
The four sites of this cohort are in northern (Ballabgarh), southern (Chennai), eastern (Kolkata) and western (Pune) parts of India. We enrolled 5336 participants across 4220 households and began surveillance in July 2018 for viral respiratory infections with additional participants enrolled annually. Trained field workers collected data about individual-level and household-level risk factors at enrolment and quarterly assessed frailty and grip strength. Trained nurses surveilled weekly to identify acute respiratory infections (ARI) and clinically assessed individuals to diagnose acute lower respiratory infection (ALRI) as per protocol. Nasal and oropharyngeal swabs are collected from all ALRI cases and one-fifth of the other ARI cases for laboratory testing. Cost data of the episode are collected using the WHO approach for estimating the economic burden of seasonal influenza. Handheld tablets with Open Data Kit platform were used for data collection.
The attrition of 352 participants due to migration and deaths was offset by enrolling 680 new entrants in the second year. All four sites reported negligible influenza vaccination uptake (0.1%-0.4%), low health insurance coverage (0.4%-22%) and high tobacco use (19%-52%). Ballabgarh had the highest proportion (54.4%) of households in the richest wealth quintile, but reported high solid fuel use (92%). Frailty levels were highest in Kolkata (11.3%) and lowest in Pune (6.8%). The Chennai cohort had highest self-reported morbidity (90.1%).
The findings of this cohort will be used to inform prioritisation of strategies for influenza and RSV control for older adults in India. We also plan to conduct epidemiological studies of SARS-CoV-2 using this platform.
我们在此描述一个针对老年人(60岁及以上)的多中心社区居住队列,该队列旨在估计印度流感和呼吸道合胞病毒(RSV)的发病率、研究风险因素、医疗保健利用情况以及经济负担。
该队列的四个研究地点分别位于印度北部(巴拉加尔)、南部(金奈)、东部(加尔各答)和西部(浦那)。我们在4220户家庭中招募了5336名参与者,并于2018年7月开始对病毒性呼吸道感染进行监测,每年还会招募更多参与者。经过培训的现场工作人员在入组时收集了关于个人层面和家庭层面风险因素的数据,并每季度评估虚弱程度和握力。经过培训的护士每周进行监测,以识别急性呼吸道感染(ARI),并根据方案对个体进行临床评估,以诊断急性下呼吸道感染(ALRI)。从所有ALRI病例以及五分之一的其他ARI病例中采集鼻拭子和口咽拭子进行实验室检测。使用世界卫生组织估计季节性流感经济负担的方法收集该疾病发作的成本数据。使用带有开放数据工具平台的手持平板电脑进行数据收集。
由于迁移和死亡导致的352名参与者流失,在第二年招募680名新参与者后得到了弥补。所有四个研究地点报告的流感疫苗接种率都极低(0.1%-0.4%),医疗保险覆盖率低(0.4%-22%),烟草使用率高(19%-52%)。巴拉加尔最富裕财富五分位数中的家庭比例最高(54.4%),但固体燃料使用率也很高(92%)。加尔各答的虚弱程度最高(11.3%),浦那最低(6.8%)。金奈队列自我报告的发病率最高(90.1%)。
该队列的研究结果将用于为印度老年人流感和RSV控制策略的优先排序提供信息。我们还计划使用这个平台对严重急性呼吸综合征冠状病毒2(SARS-CoV-2)进行流行病学研究。