Ruiz-Margáin Astrid, Román-Calleja Berenice M, Moreno-Guillén Paulina, González-Regueiro José A, Kúsulas-Delint Deyanira, Campos-Murguía Alejandro, Flores-García Nayelli C, Macías-Rodríguez Ricardo Ulises
Liver Nutrition Clinic, Department of Gastroenterology, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City 14080, Mexico.
Department of Gastroenterology, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City 14080, Mexico.
World J Gastrointest Oncol. 2021 Oct 15;13(10):1440-1452. doi: 10.4251/wjgo.v13.i10.1440.
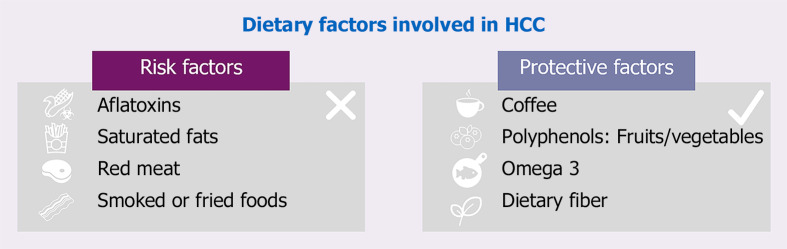
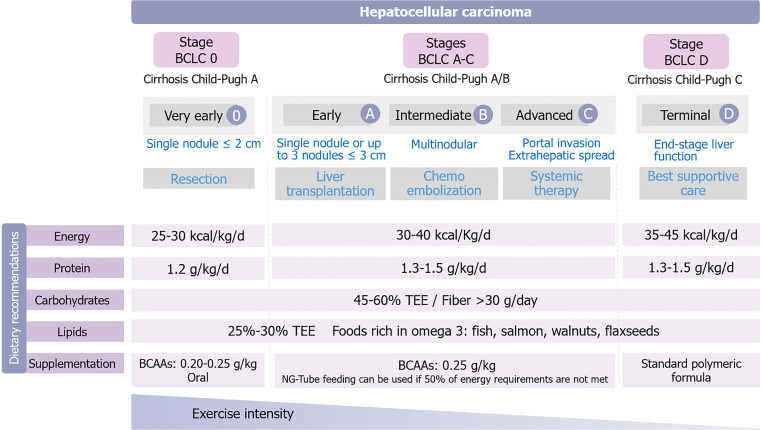
Hepatocellular carcinoma (HCC) is the most frequent primary liver cancer and presents together with cirrhosis in most cases. In addition to commonly recognized risk factors for HCC development, such as hepatitis B virus/hepatitis C virus infection, age and alcohol/tobacco consumption, there are nutritional risk factors also related to HCC development including high intake of saturated fats derived from red meat, type of cooking (generation of heterocyclic amines) and contamination of foods with aflatoxins. On the contrary, protective nutritional factors include diets rich in fiber, fruits and vegetables, n-3 polyunsaturated fatty acids and coffee. While the patient is being evaluated for staging and treatment of HCC, special attention should be paid to nutritional support, including proper nutritional assessment and therapy by a multidisciplinary team. It must be considered that these patients usually develop HCC on top of long-lasting cirrhosis, and therefore they could present with severe malnutrition. Cirrhosis-related complications should be properly addressed and considered for nutritional care. In addition to traditional methods, functional testing, phase angle and computed tomography scan derived skeletal muscle index-L3 are among the most useful tools for nutritional assessment. Nutritional therapy should be centered on providing enough energy and protein to manage the increased requirements of both cirrhosis and cancer. Supplementation with branched-chain amino acids is also recommended as it improves response to treatment, nutritional status and survival, and finally physical exercise must be encouraged and adapted to individual needs.
肝细胞癌(HCC)是最常见的原发性肝癌,多数情况下与肝硬化并存。除了公认的HCC发生风险因素,如乙型肝炎病毒/丙型肝炎病毒感染、年龄以及酒精/烟草消费外,还有与HCC发生相关的营养风险因素,包括红肉中饱和脂肪的高摄入量、烹饪方式(杂环胺的产生)以及食物被黄曲霉毒素污染。相反,具有保护作用的营养因素包括富含纤维、水果和蔬菜的饮食、n-3多不饱和脂肪酸以及咖啡。在对HCC患者进行分期评估和治疗时,应特别关注营养支持,包括由多学科团队进行适当的营养评估和治疗。必须认识到,这些患者通常在长期肝硬化的基础上发生HCC,因此可能存在严重营养不良。应妥善处理与肝硬化相关的并发症,并在营养护理中予以考虑。除传统方法外,功能测试、相位角以及计算机断层扫描得出的第三腰椎骨骼肌指数是营养评估最有用的工具之一。营养治疗应以提供足够的能量和蛋白质为核心,以满足肝硬化和癌症增加的需求。还建议补充支链氨基酸,因为它能改善治疗反应、营养状况和生存率,最后必须鼓励体育锻炼并使其适应个体需求。