Robba Chiara, Ball Lorenzo, Nogas Stefano, Battaglini Denise, Messina Antonio, Brunetti Iole, Minetti Giuseppe, Castellan Lucio, Rocco Patricia R M, Pelosi Paolo
Anesthesia and Intensive Care, San Martino Policlinico Hospital, Istituto di Ricovero e Cura a Carattere Scientifico (IRCCS) for Oncology and Neurosciences, Genoa, Italy.
Department of Surgical Sciences and Integrated Diagnostics (DISC), University of Genoa, Genoa, Italy.
Front Physiol. 2021 Oct 18;12:711273. doi: 10.3389/fphys.2021.711273. eCollection 2021.
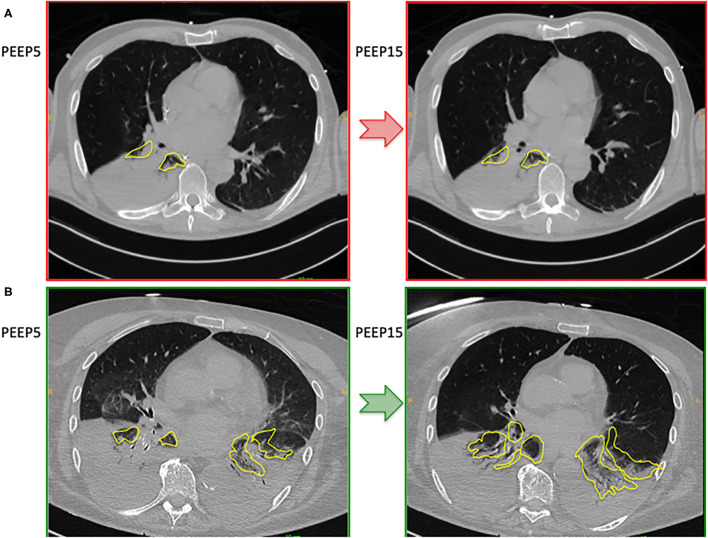
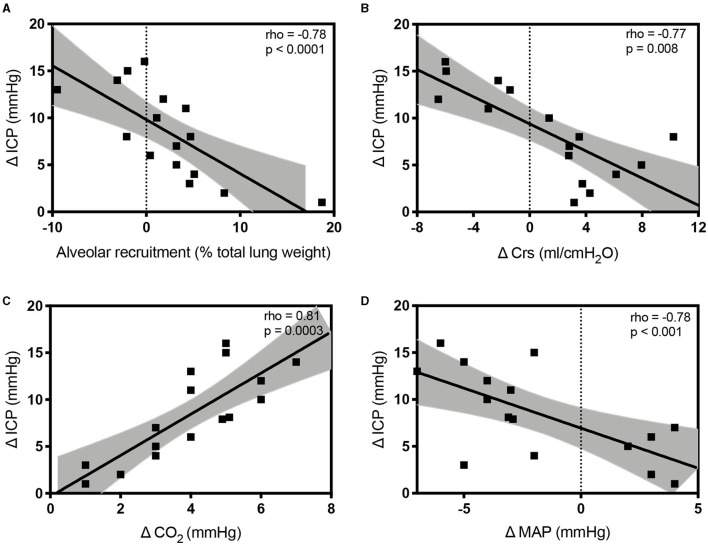
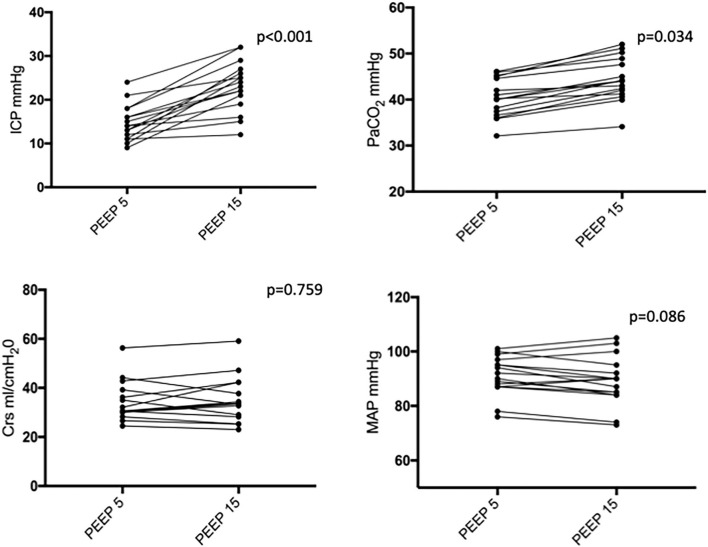
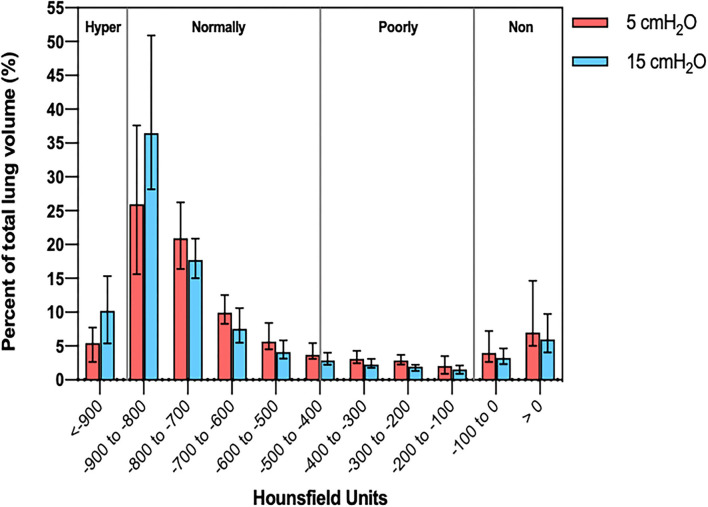
The pathophysiological effects of positive end-expiratory pressure (PEEP) on respiratory mechanics, lung recruitment, and intracranial pressure (ICP) in acute brain-injured patients have not been completely elucidated. The primary aim of this study was to assess the effects of PEEP augmentation on respiratory mechanics, quantitative computed lung tomography (qCT) findings, and its relationship with ICP modifications. Secondary aims included the assessment of the correlations between different factors (respiratory mechanics and qCT features) with the changes of ICP and how these factors at baseline may predict ICP response after greater PEEP levels. A prospective, observational study included mechanically ventilated patients with acute brain injury requiring invasive ICP and who underwent two-PEEP levels lung CT scan. Respiratory system compliance (Crs), arterial partial pressure of carbon dioxide (PaCO), mean arterial pressure (MAP), data from qCT and ICP were obtained at PEEP 5 and 15 cmHO. Sixteen examinations (double PEEP lung CT and neuromonitoring) in 15 patients were analyzed. The median age of the patients was 54 years (interquartile range, IQR = 39-65) and 53% were men. The median Glasgow Coma Scale (GCS) at intensive care unit (ICU) admission was 8 (IQR = 3-12). Median alveolar recruitment was 2.5% of total lung weight (-1.5 to 4.7). PEEP from 5 to 15 cmHO increased ICP [median values from 14.0 (11.2-17.5) to 23.5 (19.5-26.8) mmHg, < 0.001, respectively]. The amount of recruited lung tissue on CT was inversely correlated with the change (Δ) in ICP (rho = -0.78; = 0.0006). Additionally, ΔCrs (rho = -0.77, = 0.008), ΔPaCO (rho = 0.81, = 0.0003), and ΔMAP (rho = -0.64, = 0.009) were correlated with ΔICP. Baseline Crs was not predictive of ICP response to PEEP. The main factors associated with increased ICP after PEEP augmentation included reduced Crs, lower MAP and lung recruitment, and increased PaCO, but none of these factors was able to predict, at baseline, ICP response to PEEP. To assess the potential benefits of increased PEEP in patients with acute brain injury, hemodynamic status, respiratory mechanics, and lung morphology should be taken into account.
呼气末正压(PEEP)对急性脑损伤患者呼吸力学、肺复张及颅内压(ICP)的病理生理影响尚未完全阐明。本研究的主要目的是评估增加PEEP对呼吸力学、定量计算机断层肺扫描(qCT)结果的影响及其与ICP变化的关系。次要目的包括评估不同因素(呼吸力学和qCT特征)与ICP变化之间的相关性,以及这些因素在基线时如何预测更高PEEP水平后的ICP反应。一项前瞻性观察性研究纳入了需要有创ICP监测且接受了两个PEEP水平肺CT扫描的急性脑损伤机械通气患者。在PEEP为5和15 cmH₂O时获取呼吸系统顺应性(Crs)、动脉血二氧化碳分压(PaCO₂)、平均动脉压(MAP)、qCT数据和ICP。分析了15例患者的16次检查(双PEEP肺CT和神经监测)。患者的中位年龄为54岁(四分位间距,IQR = 39 - 65),53%为男性。重症监护病房(ICU)入院时格拉斯哥昏迷量表(GCS)的中位数为8(IQR = 3 - 12)。肺泡复张的中位数为肺总重量的2.5%(-1.5至4.7)。PEEP从5 cmH₂O增加到15 cmH₂O时ICP升高[中位数分别从14.0(11.2 - 17.5)mmHg升至23.5(19.5 - 26.8)mmHg,P < 0.001]。CT上肺组织复张量与ICP的变化(Δ)呈负相关(rho = -0.78;P = 0.0006)。此外,ΔCrs(rho = -0.77,P = 0.008)、ΔPaCO₂(rho = 0.81,P = 0.0003)和ΔMAP(rho = -0.64,P = 0.009)与ΔICP相关。基线Crs不能预测ICP对PEEP的反应。PEEP增加后与ICP升高相关的主要因素包括Crs降低、MAP降低、肺复张及PaCO₂升高,但这些因素在基线时均不能预测ICP对PEEP的反应。为评估增加PEEP对急性脑损伤患者的潜在益处,应考虑血流动力学状态、呼吸力学和肺形态。