O'Dowd Timothy R, Mc Hugh Jack W, Theel Elitza S, Wengenack Nancy L, O'Horo John C, Enzler Mark J, Vergidis Paschalis
Department of Medicine, Mayo Clinic, Rochester, MN 55905, USA.
Department of Laboratory Medicine and Pathology, Division of Clinical Microbiology, Mayo Clinic, Rochester, MN 55905, USA.
J Fungi (Basel). 2021 Oct 20;7(11):888. doi: 10.3390/jof7110888.
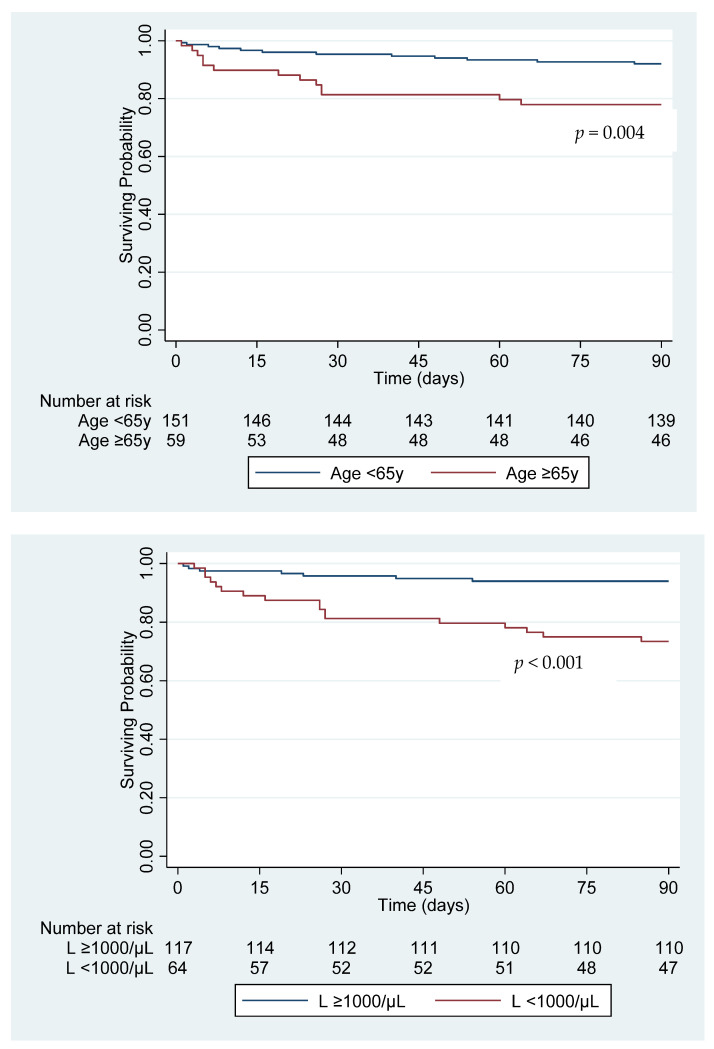
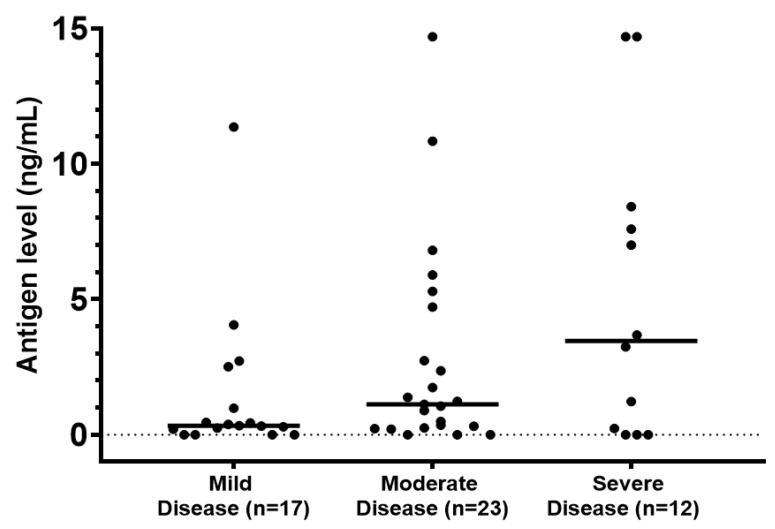
Blastomycosis can cause severe disease with progressive respiratory failure and dissemination even in immunocompetent individuals. We sought to evaluate risk factors for severe disease and mortality using clinical and laboratory data within a large health system in an endemic area. We performed a retrospective cohort study of patients diagnosed with blastomycosis at all Mayo Clinic sites from 1 January 2004 through 31 March 2020. Diagnosis was established by culture, histopathology/cytopathology, serology, antigen testing, or PCR. Disease was categorized as mild for patients treated in the outpatient setting, moderate for hospitalized patients who did not require intensive care, and severe for patients admitted to the intensive care unit. Logistic regression was used to evaluate risk factors for severe disease. A Cox proportional hazards model was constructed to evaluate mortality. We identified 210 patients diagnosed with blastomycosis. Mean age was 51 years (range, 6-84). Most subjects were male (71.0%). Extrapulmonary disease was confirmed in 24.8%. In this cohort, 40.5% of patients had mild disease, 37.6% had moderate disease, and 21.9% had severe disease. Independent risk factors for severe disease were neutrophilia (odds ratio (OR) 3.35 (95% CI 1.53-7.35), = 0.002) and lymphopenia (OR 3.34 (95% CI 1.59-7.03), = 0.001). Mortality at 90 days was 11.9%. Median time from diagnosis to death was 23 days (interquartile range 8-31 days). Independent risk factors for mortality were age (OR 1.04 (95% CI 1.01-1.08), = 0.009), neutrophilia (OR 2.84 (95% CI 1.04-7.76), = 0.041), and lymphopenia (OR 4.50 (95% CI 1.67-12.11), = 0.003). immunodiffusion had an overall sensitivity of 39.6% (95% CI 30.1-49.8). Sensitivity was higher among those who were tested 4 weeks or longer after the onset of symptoms. Urine antigen had a significantly higher sensitivity of 80.8% (95% CI 68.1-89.2) compared to serology. There was a trend towards higher antigen concentration in patients with severe disease. The sensitivity of PCR from respiratory specimens was 67.6% (95% CI 50.1-85.5). In this cohort, we did not find an association between pharmacologic immunosuppression and disease severity. Lymphopenia at diagnosis was an independent risk factor for mortality. This simple marker may aid clinicians in determining disease prognosis.
芽生菌病即使在免疫功能正常的个体中也可导致严重疾病,并伴有进行性呼吸衰竭和播散。我们试图利用流行地区一个大型医疗系统内的临床和实验室数据,评估严重疾病和死亡的危险因素。我们对2004年1月1日至2020年3月31日在梅奥诊所所有院区被诊断为芽生菌病的患者进行了一项回顾性队列研究。通过培养、组织病理学/细胞病理学、血清学、抗原检测或聚合酶链反应(PCR)确诊。对于在门诊接受治疗的患者,疾病分类为轻度;对于不需要重症监护的住院患者,疾病分类为中度;对于入住重症监护病房的患者,疾病分类为重度。采用逻辑回归评估严重疾病的危险因素。构建Cox比例风险模型评估死亡率。我们确定了210例被诊断为芽生菌病的患者。平均年龄为51岁(范围6 - 84岁)。大多数受试者为男性(71.0%)。肺外疾病确诊率为24.8%。在该队列中,40.5%的患者患有轻度疾病,37.6%患有中度疾病,21.9%患有重度疾病。严重疾病的独立危险因素为中性粒细胞增多(比值比(OR)3.35(95%置信区间1.53 - 7.35),P = 0.002)和淋巴细胞减少(OR 3.34(95%置信区间1.59 - 7.03),P = 0.001)。90天死亡率为11.9%。从诊断到死亡的中位时间为23天(四分位间距8 - 31天)。死亡的独立危险因素为年龄(OR 1.04(95%置信区间1.01 - 1.08),P = 0.009)、中性粒细胞增多(OR 2.84(95%置信区间1.04 - 7.76),P = 0.041)和淋巴细胞减少(OR 4.50(95%置信区间1.67 - 12.11),P = 0.003)。免疫扩散的总体敏感性为39.6%(95%置信区间30.1 - 49.8)。在症状出现4周或更长时间后接受检测的人群中,敏感性更高。与血清学相比,尿抗原的敏感性显著更高,为80.8%(95%置信区间68.1 - 89.2)。重症患者的抗原浓度有升高趋势。呼吸道标本PCR的敏感性为67.6%(95%置信区间50.1 - 85.5)。在该队列中,我们未发现药物性免疫抑制与疾病严重程度之间存在关联。诊断时淋巴细胞减少是死亡的独立危险因素。这个简单指标可能有助于临床医生确定疾病预后。