Department of Medical Microbiology, School of Laboratory Medicine & Medical Sciences, Howard College, University of KwaZulu-Natal, Glenwood, Durban, 4041, South Africa.
Division of Research Capacity Development, South African Medical Research Council (SAMRC), Tygerberg, Cape Town, 7505, South Africa.
Global Health. 2022 Jan 22;18(1):5. doi: 10.1186/s12992-022-00796-7.
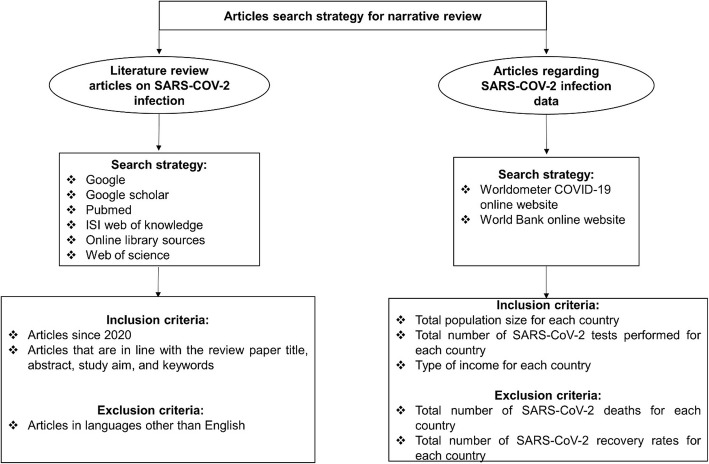
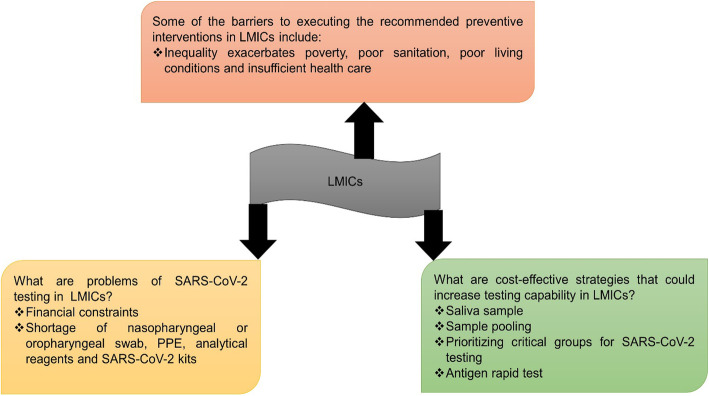
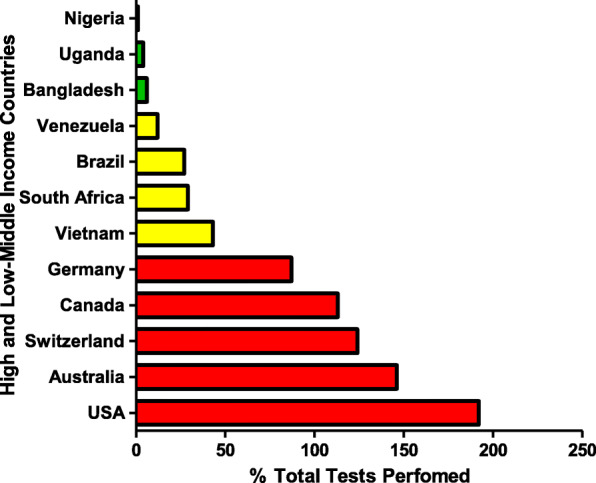
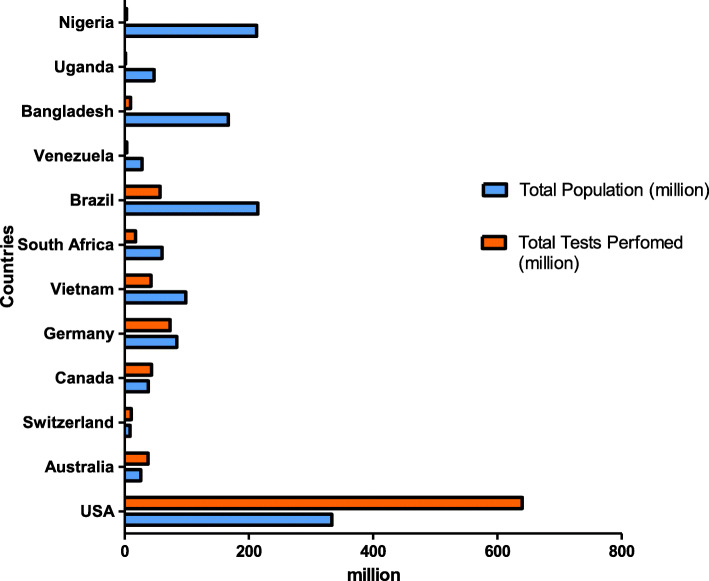
Diagnostic testing for the Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection remains a challenge around the world, especially in low-middle-income countries (LMICs) with poor socio-economic backgrounds. From the beginning of the pandemic in December 2019 to August 2021, a total of approximately 3.4 billion tests were performed globally. The majority of these tests were restricted to high income countries. Reagents for diagnostic testing became a premium, LMICs either cannot afford or find manufacturers unwilling to supply them with expensive analytical reagents and equipment. From March to December 2020 obtaining testing kits for SARS-CoV-2 testing was a challenge. As the number of SARS-CoV-2 infection cases increases globally, large-scale testing still remains a challenge in LMICs. The aim of this review paper is to compare the total number and frequencies of SARS-CoV-2 testing in LMICs and high-income countries (HICs) using publicly available data from Worldometer COVID-19, as well as discussing possible interventions and cost-effective measures to increase testing capability in LMICs. In summary, HICs conducted more SARS-CoV-2 testing (USA: 192%, Australia: 146%, Switzerland: 124% and Canada: 113%) compared to middle-income countries (MICs) (Vietnam: 43%, South Africa: 29%, Brazil: 27% and Venezuela: 12%) and low-income countries (LICs) (Bangladesh: 6%, Uganda: 4% and Nigeria: 1%). Some of the cost-effective solutions to counteract the aforementioned problems includes using saliva instead of oropharyngeal or nasopharyngeal swabs, sample pooling, and testing high-priority groups to increase the number of mass testing in LMICs.
诊断严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染的检测在全球范围内仍然是一个挑战,尤其是在社会经济背景较差的中低收入国家(LMICs)。自 2019 年 12 月大流行开始到 2021 年 8 月,全球共进行了约 34 亿次检测。这些检测大多数仅限于高收入国家。诊断检测试剂成为一种奢侈品,中低收入国家要么负担不起,要么发现制造商不愿意向他们供应昂贵的分析试剂和设备。2020 年 3 月至 12 月,获得 SARS-CoV-2 检测试剂盒是一个挑战。随着全球 SARS-CoV-2 感染病例的增加,大规模检测在中低收入国家仍然是一个挑战。本文的目的是使用 Worldometer COVID-19 上的公开数据比较中低收入国家和高收入国家(HICs)进行的 SARS-CoV-2 检测的总数和频率,并讨论增加中低收入国家检测能力的可能干预措施和具有成本效益的措施。总的来说,与中等收入国家(MICs)(越南:43%,南非:29%,巴西:27%和委内瑞拉:12%)和低收入国家(LICs)(孟加拉国:6%,乌干达:4%和尼日利亚:1%)相比,高收入国家(HICs)进行了更多的 SARS-CoV-2 检测(美国:192%,澳大利亚:146%,瑞士:124%和加拿大:113%)。一些具有成本效益的解决方案包括使用唾液代替鼻咽或口咽拭子、样本混合以及对高优先级人群进行检测,以增加中低收入国家的大规模检测数量。