Cardiac Department, Hospital Universitario Virgen de la Arrixaca, Murcia, Spain.
Cardiogenetic Laboratory, Instituto Murciano de Investigación Biosanitaria, Murcia, Spain.
PLoS One. 2022 Feb 4;17(2):e0263140. doi: 10.1371/journal.pone.0263140. eCollection 2022.
Infection by the SARS-Cov-2 virus produces in humans a disease of highly variable and unpredictable severity. The presence of frequent genetic single nucleotide polymorphisms (SNPs) in the population might lead to a greater susceptibility to infection or an exaggerated inflammatory response. SARS-CoV-2 requires the presence of the ACE2 protein to enter in the cell and ACE2 is a regulator of the renin-angiotensin system. Accordingly, we studied the associations between 8 SNPs from AGTR1, ACE2 and ACE genes and the severity of the disease produced by the SARS-Cov-2 virus.
318 (aged 59.6±17.3 years, males 62.6%) COVID-19 patients were grouped based on the severity of symptoms: Outpatients (n = 104, 32.7%), hospitalized on the wards (n = 73, 23.0%), Intensive Care Unit (ICU) (n = 84, 26.4%) and deceased (n = 57, 17.9%). Comorbidity data (diabetes, hypertension, obesity, lung disease and cancer) were collected for adjustment. Genotype distribution of 8 selected SNPs among the severity groups was analyzed.
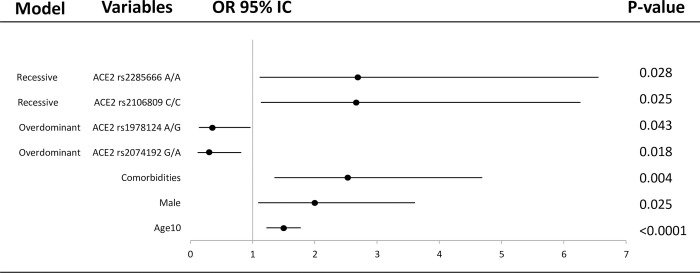
Four SNPs in ACE2 were associated with the severity of disease. While rs2074192 andrs1978124showed a protector effectassuming an overdominant model of inheritance (G/A vs. GG-AA, OR = 0.32, 95%CI = 0.12-0.82; p = 0.016 and A/G vs. AA-GG, OR = 0.37, 95%CI: 0.14-0.96; p = 0.038, respectively); the SNPs rs2106809 and rs2285666were associated with an increased risk of being hospitalized and a severity course of the disease with recessive models of inheritance (C/C vs. T/C-T/T, OR = 11.41, 95% CI: 1.12-115.91; p = 0.012) and (A/A vs. GG-G/A, OR = 12.61, 95% CI: 1.26-125.87; p = 0.0081). As expected, an older age (OR = 1.47), male gender (OR = 1.98) and comorbidities (OR = 2.52) increased the risk of being admitted to ICU or death vs more benign outpatient course. Multivariable analysis demonstrated the role of the certain genotypes (ACE2) with the severity of COVID-19 (OR: 0.31, OR 0.37 for rs2074192 and rs1978124, and OR = 2.67, OR = 2.70 for rs2106809 and rs2285666, respectively). Hardy-Weinberg equilibrium in hospitalized group for I/D SNP in ACE was not showed (p<0.05), which might be due to the association with the disease. No association between COVID-19 disease and the different AGTR1 SNPs was evidenced on multivariable, nevertheless the A/A genotype for rs5183 showed an higher hospitalization risk in patients with comorbidities.
Different genetic variants in ACE2 were associated with a severe clinical course and death groups of patients with COVID-19. ACE2 common SNPs in the population might modulate severity of COVID-19 infection independently of other known markers like gender, age and comorbidities.
SARS-CoV-2 病毒感染会导致人类疾病的严重程度高度变化和不可预测。人群中频繁出现的单核苷酸基因多态性(SNP)可能会导致更高的易感性或更严重的炎症反应。SARS-CoV-2 需要 ACE2 蛋白进入细胞,ACE2 是肾素-血管紧张素系统的调节剂。因此,我们研究了 AGTR1、ACE2 和 ACE 基因中的 8 个 SNP 与 SARS-CoV-2 病毒引起的疾病严重程度之间的关系。
根据症状严重程度将 318 名(年龄 59.6±17.3 岁,男性 62.6%)COVID-19 患者分为以下组:门诊患者(n=104,32.7%)、住院病房(n=73,23.0%)、重症监护病房(n=84,26.4%)和死亡(n=57,17.9%)。收集了合并症(糖尿病、高血压、肥胖、肺部疾病和癌症)数据进行调整。分析了严重程度组中 8 个选定 SNP 的基因型分布。
ACE2 中的 4 个 SNP 与疾病严重程度相关。虽然 rs2074192 和 rs1978124 显示出保护作用,假设为超显性遗传模式(G/A 与 GG-AA,OR=0.32,95%CI=0.12-0.82;p=0.016 和 A/G 与 AA-GG,OR=0.37,95%CI:0.14-0.96;p=0.038);SNP rs2106809 和 rs2285666 与住院风险增加和疾病严重程度呈隐性遗传模式相关(C/C 与 T/C-T/T,OR=11.41,95%CI:1.12-115.91;p=0.012)和(A/A 与 GG-G/A,OR=12.61,95%CI:1.26-125.87;p=0.0081)。正如预期的那样,年龄较大(OR=1.47)、男性(OR=1.98)和合并症(OR=2.52)增加了 ICU 或死亡的风险,而良性门诊患者的风险则较低。多变量分析表明了某些基因型(ACE2)与 COVID-19 严重程度的作用(OR:0.31,OR 0.37 用于 rs2074192 和 rs1978124,OR=2.67,OR=2.70 用于 rs2106809 和 rs2285666)。ACE 中的 I/D SNP 在住院组中未显示 Hardy-Weinberg 平衡(p<0.05),这可能与疾病有关。多变量分析未显示 COVID-19 疾病与不同的 AGTR1 SNP 之间存在关联,但 rs5183 的 A/A 基因型在合并症患者中显示出更高的住院风险。
ACE2 中的不同遗传变异与 COVID-19 患者的严重临床病程和死亡组相关。人群中 ACE2 的常见 SNP 可能独立于性别、年龄和合并症等其他已知标志物,调节 COVID-19 感染的严重程度。