Division of Gastroenterology, University of California San Diego School of Medicine, La Jolla, California.
Division of Gastroenterology, Washington University School of Medicine, St. Louis, Missouri.
Clin Gastroenterol Hepatol. 2022 May;20(5):984-994.e1. doi: 10.1016/j.cgh.2022.01.025. Epub 2022 Feb 2.
BACKGROUND & AIMS: As many as one-half of all patients with suspected gastroesophageal reflux disease (GERD) do not derive benefit from acid suppression. This review outlines a personalized diagnostic and therapeutic approach to GERD symptoms.
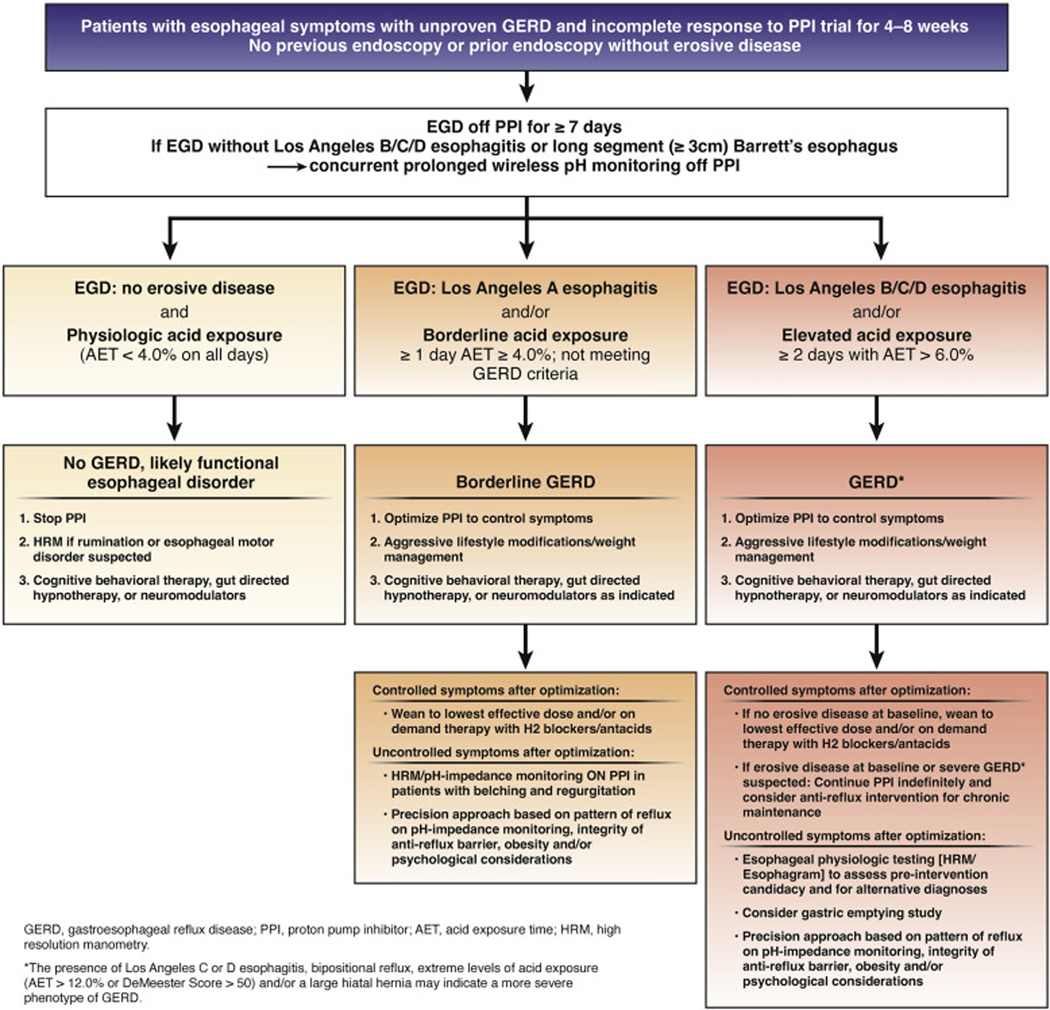
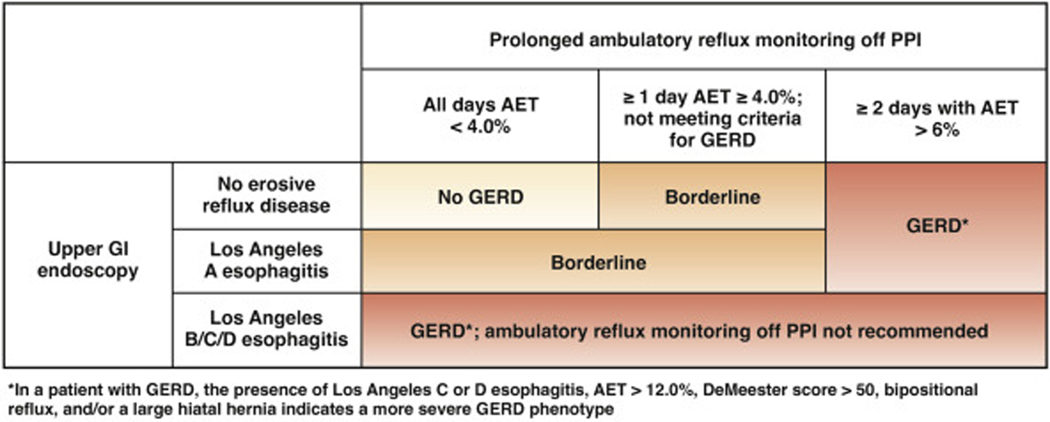
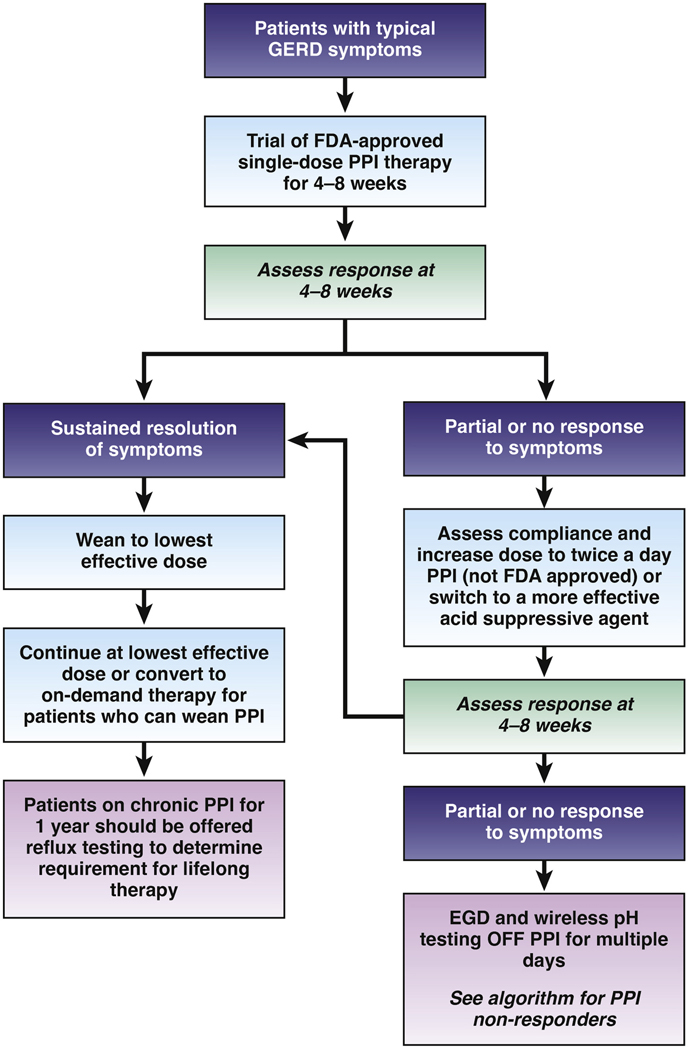
The Best Practice Advice statements presented here were developed from expert review of existing literature combined with extensive discussion and expert opinion to provide practical advice. Formal rating of the quality of evidence or strength of recommendations was not the intent of this clinical practice update. BEST PRACTICE ADVICE 1: Clinicians should develop a care plan for investigation of symptoms suggestive of GERD, selection of therapy (with explanation of potential risks and benefits), and long-term management, including possible de-escalation, in a shared-decision making model with the patient. BEST PRACTICE ADVICE 2: Clinicians should provide standardized educational material on GERD mechanisms, weight management, lifestyle and dietary behaviors, relaxation strategies, and awareness about the brain-gut axis relationship to patients with reflux symptoms. BEST PRACTICE ADVICE 3: Clinicians should emphasize safety of proton pump inhibitors (PPIs) for the treatment of GERD. BEST PRACTICE ADVICE 4: Clinicians should provide patients presenting with troublesome heartburn, regurgitation, and/or non-cardiac chest pain without alarm symptoms a 4- to 8-week trial of single-dose PPI therapy. With inadequate response, dosing can be increased to twice a day or switched to a more effective acid suppressive agent once a day. When there is adequate response, PPI should be tapered to the lowest effective dose. BEST PRACTICE ADVICE 5: If PPI therapy is continued in a patient with unproven GERD, clinicians should evaluate the appropriateness and dosing within 12 months after initiation, and offer endoscopy with prolonged wireless reflux monitoring off PPI therapy to establish appropriateness of long-term PPI therapy. BEST PRACTICE ADVICE 6: If troublesome heartburn, regurgitation, and/or non-cardiac chest pain do not respond adequately to a PPI trial or when alarm symptoms exist, clinicians should investigate with endoscopy and, in the absence of erosive reflux disease (Los Angeles B or greater) or long-segment (≥3 cm) Barrett's esophagus, perform prolonged wireless pH monitoring off medication (96-hour preferred if available) to confirm and phenotype GERD or to rule out GERD. BEST PRACTICE ADVICE 7: Complete endoscopic evaluation of GERD symptoms includes inspection for erosive esophagitis (graded according to the Los Angeles classification when present), diaphragmatic hiatus (Hill grade of flap valve), axial hiatus hernia length, and inspection for Barrett's esophagus (graded according to the Prague classification and biopsied when present). BEST PRACTICE ADVICE 8: Clinicians should perform upfront objective reflux testing off medication (rather than an empiric PPI trial) in patients with isolated extra-esophageal symptoms and suspicion for reflux etiology. BEST PRACTICE ADVICE 9: In symptomatic patients with proven GERD, clinicians should consider ambulatory 24-hour pH-impedance monitoring on PPI as an option to determine the mechanism of persisting esophageal symptoms despite therapy (if adequate expertise exists for interpretation). BEST PRACTICE ADVICE 10: Clinicians should personalize adjunctive pharmacotherapy to the GERD phenotype, in contrast to empiric use of these agents. Adjunctive agents include alginate antacids for breakthrough symptoms, nighttime H2 receptor antagonists for nocturnal symptoms, baclofen for regurgitation or belch predominant symptoms, and prokinetics for coexistent gastroparesis. BEST PRACTICE ADVICE 11: Clinicians should provide pharmacologic neuromodulation, and/or referral to a behavioral therapist for hypnotherapy, cognitive behavioral therapy, diaphragmatic breathing, and relaxation strategies in patients with functional heartburn or reflux disease associated with esophageal hypervigilance reflux hypersensitivity and/or behavioral disorders. BEST PRACTICE ADVICE 12: In patients with proven GERD, laparoscopic fundoplication and magnetic sphincter augmentation are effective surgical options, and transoral incisionless fundoplication is an effective endoscopic option in carefully selected patients. BEST PRACTICE ADVICE 13: In patients with proven GERD, Roux-en-Y gastric bypass is an effective primary anti-reflux intervention in obese patients, and a salvage option in non-obese patients, whereas sleeve gastrectomy has potential to worsen GERD. BEST PRACTICE ADVICE 14: Candidacy for invasive anti-reflux procedures includes confirmatory evidence of pathologic GERD, exclusion of achalasia, and assessment of esophageal peristaltic function.
多达一半的疑似胃食管反流病(GERD)患者不能从抑酸治疗中获益。本综述概述了 GERD 症状的个性化诊断和治疗方法。
这里提出的最佳实践建议陈述是通过专家对现有文献的审查以及广泛的讨论和专家意见来制定的,旨在提供实用建议。本临床实践更新并未旨在对证据质量或推荐强度进行正式评级。最佳实践建议 1:临床医生应制定针对 GERD 症状的调查、治疗选择(解释潜在风险和益处)以及长期管理计划,包括可能的降级,以与患者共同决策。最佳实践建议 2:临床医生应向有反流症状的患者提供关于 GERD 机制、体重管理、生活方式和饮食行为、放松策略以及对大脑-肠道轴关系的认识的标准化教育材料。最佳实践建议 3:临床医生应强调质子泵抑制剂(PPIs)治疗 GERD 的安全性。最佳实践建议 4:对于出现烦人的烧心、反流和/或非心源性胸痛且无警报症状的患者,临床医生应给予 4-8 周的单剂量 PPI 治疗试验。如果反应不足,可以增加剂量至每天两次,或更换更有效的抑酸剂每天一次。当反应充分时,应将 PPI 逐渐减少至最低有效剂量。最佳实践建议 5:如果在未经证实的 GERD 患者中继续使用 PPI 治疗,临床医生应在开始后 12 个月内评估其适当性和剂量,并提供在 PPI 治疗之外进行内镜检查和延长无线反流监测,以确定长期 PPI 治疗的适当性。最佳实践建议 6:如果烦人的烧心、反流和/或非心源性胸痛不能通过 PPI 试验充分缓解,或者存在警报症状,临床医生应进行内镜检查,如果没有糜烂性反流病(洛杉矶 B 或更高级别)或长段(≥3 厘米)巴雷特食管,在药物治疗之外进行延长无线 pH 监测(如果有 96 小时则首选),以确认和表现 GERD 或排除 GERD。最佳实践建议 7:GERD 症状的完整内镜评估包括检查糜烂性食管炎(如有存在,根据洛杉矶分类分级)、横膈裂孔(瓣阀的 Hill 分级)、轴向裂孔疝长度以及巴雷特食管检查(根据布拉格分类分级,如有存在则进行活检)。最佳实践建议 8:对于有孤立性食管外症状和怀疑反流病因的患者,临床医生应在开始时进行药物治疗之外的客观反流测试(而不是经验性 PPI 试验)。最佳实践建议 9:对于已确诊的 GERD 患者,在有症状的患者中,如果存在治疗后食管症状持续存在的情况,临床医生应考虑在 PPI 治疗之外进行 24 小时 pH 阻抗监测,以确定其机制(如果有足够的专业知识进行解释)。最佳实践建议 10:临床医生应根据 GERD 表型个体化辅助药物治疗,而不是经验性使用这些药物。辅助药物包括用于突破性症状的藻酸盐抗酸剂、用于夜间症状的夜间 H2 受体拮抗剂、用于反流或嗳气为主症状的巴氯芬,以及用于并存胃轻瘫的促动力药。最佳实践建议 11:临床医生应提供药物神经调节,并/或将患者转介给行为治疗师,进行催眠治疗、认知行为治疗、膈式呼吸和放松策略,用于功能性烧心或与食管高敏性反流、过度敏感和/或行为障碍相关的反流性疾病。最佳实践建议 12:在已确诊的 GERD 患者中,腹腔镜胃底折叠术和磁括约肌增强术是有效的手术选择,经口无切口胃底折叠术是精心选择患者的有效内镜选择。最佳实践建议 13:在已确诊的 GERD 患者中,肥胖患者的 Roux-en-Y 胃旁路手术是一种有效的原发性抗反流干预措施,在非肥胖患者中是一种补救选择,而袖状胃切除术有加重 GERD 的潜力。最佳实践建议 14:侵入性抗反流手术的候选者包括病理性 GERD 的确认证据、排除贲门失弛缓症以及食管蠕动功能的评估。