Sheffield Dermatology Research, Department of Infection, Immunity and Cardiovascular Disease, University of Sheffield Medical School, Sheffield, UK.
Statistical Services Unit, University of Sheffield, Sheffield, UK.
Clin Exp Dermatol. 2022 Jun;47(6):1154-1164. doi: 10.1111/ced.15141. Epub 2022 Apr 12.
Eczema (atopic dermatitis; AD) is a very common itchy skin condition affecting 1 in 5 children and up to 1 in 10 adults worldwide. The skin of eczema sufferers is prone to redness, irritation and dryness because it does not form an effective barrier, i.e. the ability of the skin to stop irritants, allergens and microorganisms getting into the body. Skin barrier dysfunction is a hallmark of AD. The regular and liberal (600 g/week for an adult) use of emollients is recommended for all patients with eczema), even between episodes of itching and redness, to soften and soothe the skin. In England alone, almost 9 million prescriptions for emollient creams were issued in 2018, at a cost of over £50 million. Despite this widespread use, relatively little is known about how commonly prescribed emollient creams affect the skin's barrier, and thus the role of moisturizers in AD development and progression remains unclear. We set out to compare three different types of emollient cream and a no-treatment control.
To compare the barrier-strengthening properties of a new moisturizer containing urea and glycerol (urea-glycerol cream; UGC), with those of a glycerol-containing moisturizer (glycerol cream; GC), a simple paraffin cream (PC) with no humectant, and a no-treatment control (NTC).
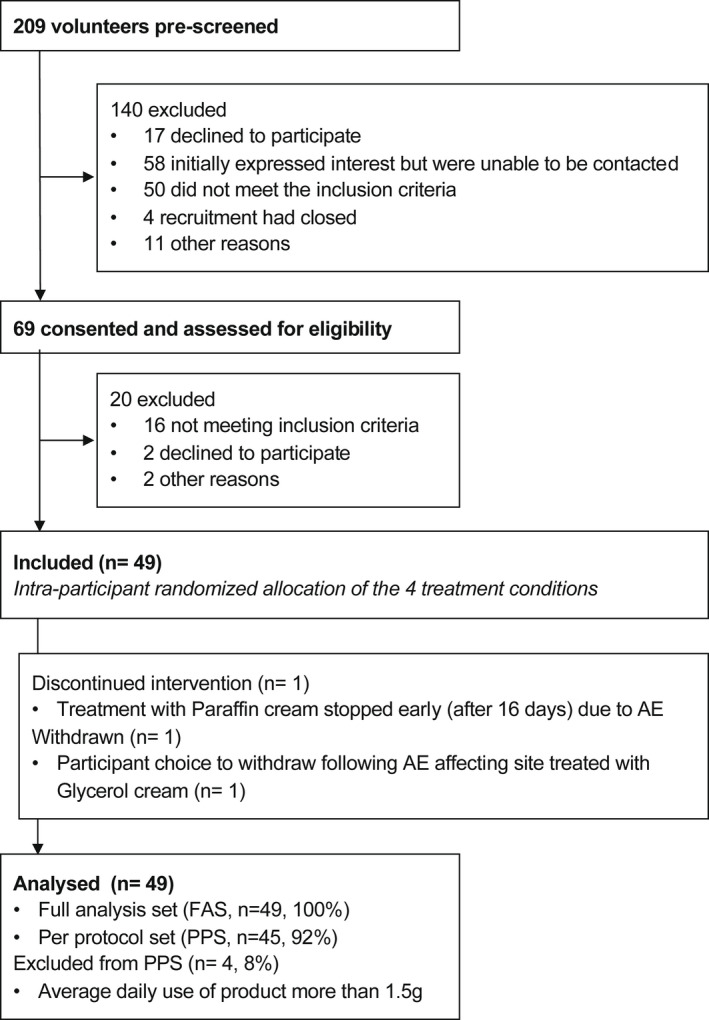
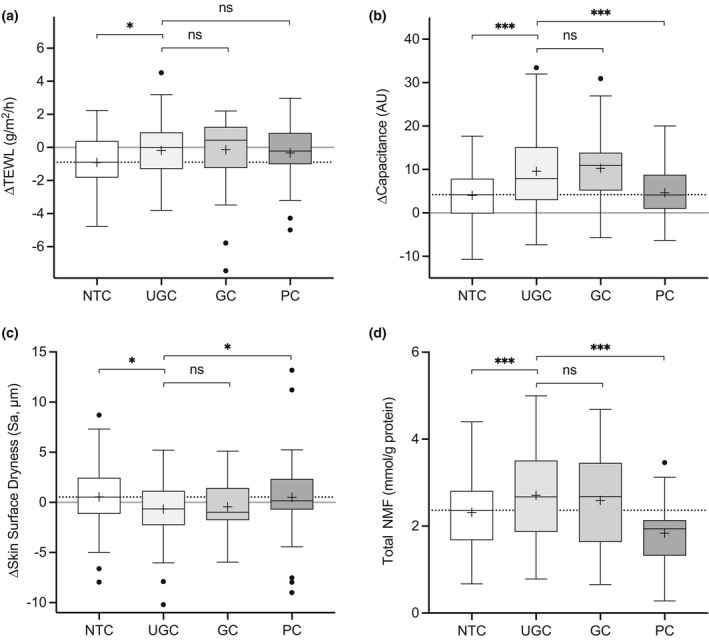
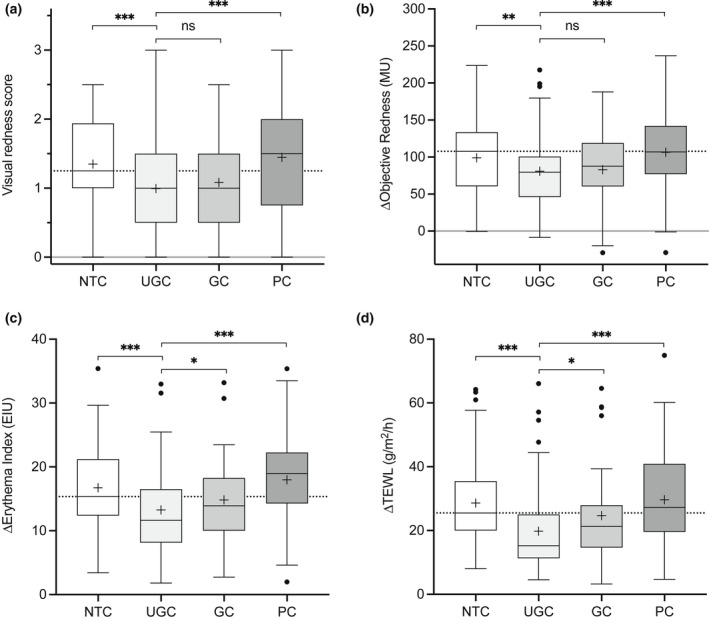
This was an observer-blinded prospective Phase 2 within-subject multilateral single-centre randomized controlled trial in adults with AD (Clinical Trials #NCT03901144). The intervention involved 4 weeks of treatment, twice daily, with the three products applied to one of four areas on the forearms the (the fourth area was the untreated control, randomized allocation). Skin properties [dryness, transepidermal water loss (TEWL), hydration and natural moisturizing factor (NMF) levels] were assessed before, during and after treatment to see what happened to the skin's barrier. The primary outcome was skin sensitivity to the irritant sodium lauryl sulfate (SLS) after treatment. We performed tests on the skin before and after treatment to see what happened to the skin's barrier.
In total, 49 patients were randomized, completed treatment and included in the analysis. UGC significantly reduced the response to SLS as indicated by a reduction in TEWL compared with NTC (-9.0 g/m /h; 95% CI -12.56 to -5.49), with PC (-9.0 g/m /h; 95% CI -12.60 to -5.44) and with GC -4.2 g/m /h; 95% CI 7.76 to -0.63). Skin moisturization improved at sites treated with UGC compared with NTC and PC, and this was accompanied by concordant changes in dryness and NMF levels. Subgroup analysis suggested FLG-dependent enhancement of treatment effects.
The study showed that not all emollient creams for eczema are equal. The simple paraffin-based emollient, which represents the most widely prescribed type of emollient cream in England, had no effect on the skin's barrier and reduced the skin's NMF. UGC markedly improved the skin's barrier and protected against irritation. GC performed better than PC, but not as well as UGC. UGC strengthened the skin barrier through a mechanism involving increased NMF levels in the skin, and imparted protection from SLS-induced irritation. By helping correct a major pathophysiological process, UGC has the potential to improve the long-term control of AD. The results show that different emollient creams have different effects on our skin, and only certain types have the ability to improve the skin's barrier and protect against irritants that trigger eczema.
湿疹(特应性皮炎;AD)是一种非常常见的瘙痒性皮肤病,影响全球 1/5 的儿童和多达 1/10 的成年人。湿疹患者的皮肤容易发红、刺激和干燥,因为它不能形成有效的屏障,即皮肤阻止刺激物、过敏原和微生物进入身体的能力。皮肤屏障功能障碍是 AD 的一个标志。建议所有湿疹患者(即使在瘙痒和发红发作之间)定期和大量(成人每周 600 克)使用保湿剂,以使皮肤柔软和舒缓。仅在英格兰,2018 年就开出了近 900 万份保湿霜处方,费用超过 5000 万英镑。尽管这种广泛的使用,但相对较少了解处方保湿剂如何影响皮肤屏障,因此保湿剂在 AD 发展和进展中的作用仍然不清楚。我们着手比较三种不同类型的保湿霜和一种无治疗对照。
比较含有尿素和甘油的新型保湿剂(尿素-甘油霜;UGC)与含有甘油的保湿剂(甘油霜;GC)、不含保湿剂的简单凡士林霜(PC)和无治疗对照(NTC)在增强皮肤屏障方面的特性。
这是一项在成年 AD 患者中进行的观察者盲前瞻性 2 期多中心随机对照试验(临床试验 #NCT03901144)。干预措施包括 4 周的治疗,每天两次,将三种产品中的一种涂抹在前臂的四个区域之一(第四个区域为未治疗的对照,随机分配)。在治疗前、治疗中和治疗后评估皮肤特性[干燥、经表皮水分流失(TEWL)、水合作用和天然保湿因子(NMF)水平],以了解皮肤屏障的变化情况。主要结局是治疗后皮肤对刺激性十二烷基硫酸钠(SLS)的敏感性。我们在治疗前后对皮肤进行了测试,以了解皮肤屏障的变化情况。
共有 49 名患者被随机分配,完成了治疗并纳入了分析。与 NTC 相比,UGC 显著降低了 SLS 的反应,表现为 TEWL 降低(-9.0 g/m/h;95%CI -12.56 至 -5.49),与 PC(-9.0 g/m/h;95%CI -12.60 至 -5.44)和 GC 相比,GC 减少了 4.2 g/m/h;95%CI 7.76 至 -0.63)。与 NTC 和 PC 相比,UGC 治疗部位的皮肤保湿性得到改善,同时干燥和 NMF 水平也发生了相应变化。亚组分析表明,FLG 依赖性增强了治疗效果。
该研究表明,并非所有治疗湿疹的保湿剂都是一样的。在英格兰最广泛开处方的简单凡士林保湿剂对皮肤屏障没有影响,反而降低了皮肤的 NMF。UGC 显著改善了皮肤屏障,并能预防刺激。GC 的效果优于 PC,但不如 UGC。UGC 通过增加皮肤中 NMF 水平来增强皮肤屏障,并提供对 SLS 诱导的刺激的保护。通过帮助纠正主要的病理生理过程,UGC 有可能改善 AD 的长期控制。结果表明,不同的保湿霜对我们的皮肤有不同的影响,只有某些类型的保湿霜具有改善皮肤屏障和防止引发湿疹的刺激物的能力。