School of Sport Science, Beijing Sport University, Beijing, China.
Key Laboratory of the Ministry of Education of Exercise and Physical Fitness, Beijing Sport University, Beijing, China.
PLoS One. 2022 Feb 15;17(2):e0263918. doi: 10.1371/journal.pone.0263918. eCollection 2022.
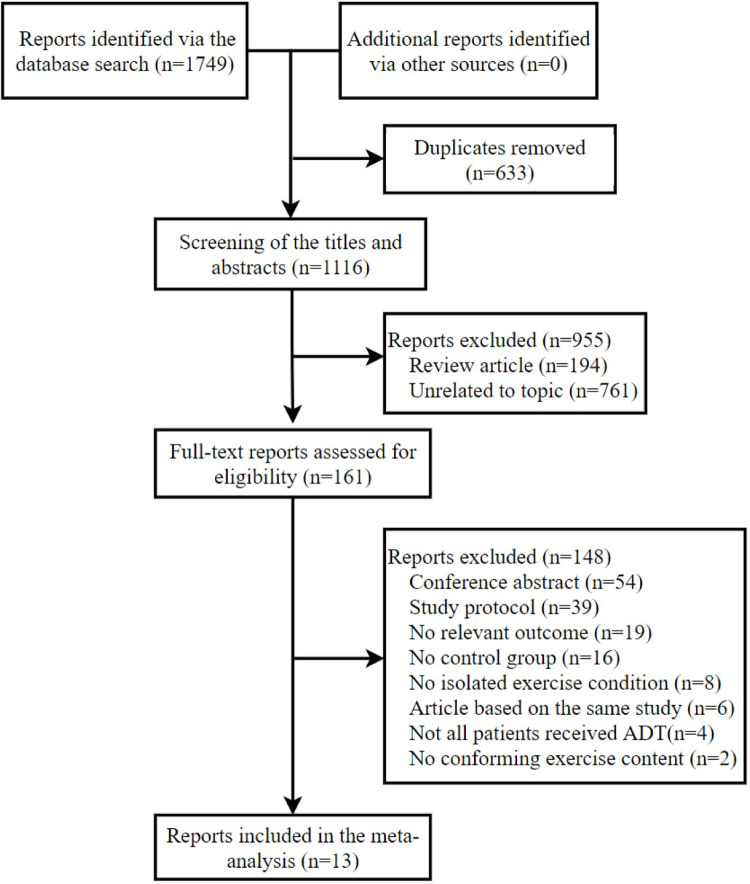
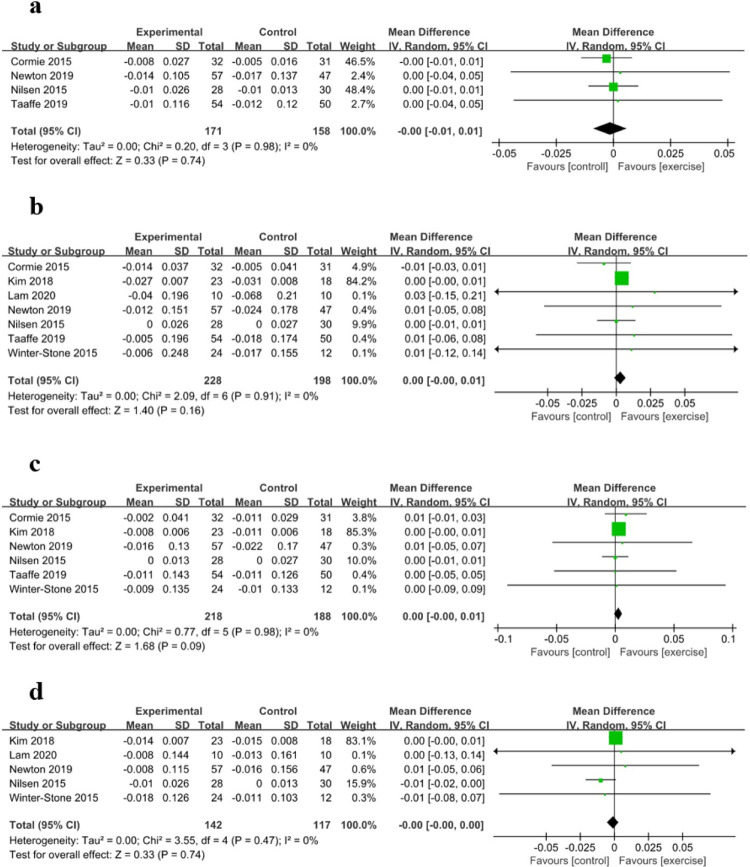
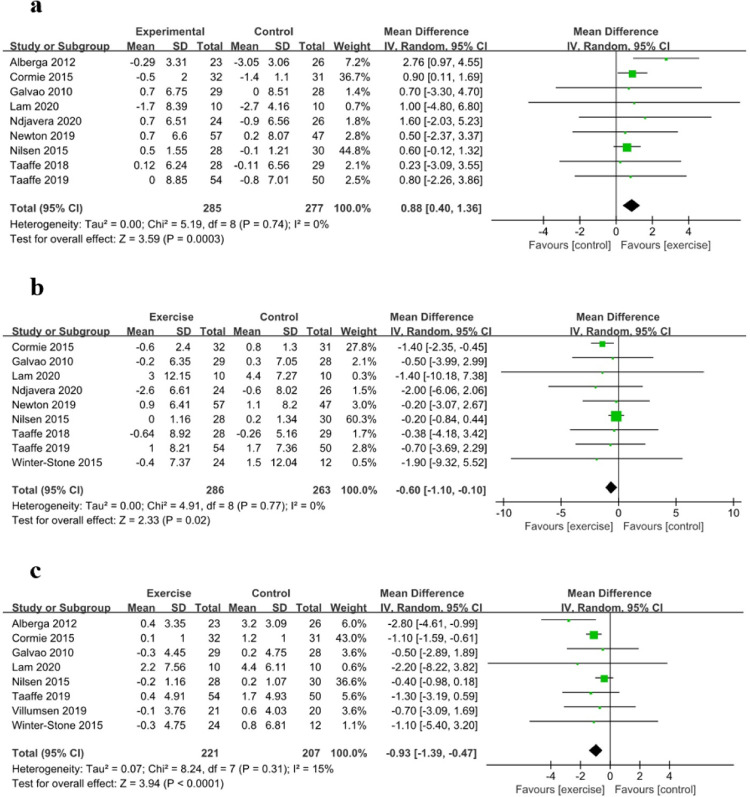
Androgen deprivation therapy is a common treatment for prostate cancer. However, this therapy is associated with various adverse effects, such as increased body fat and decreased bone mineral density. Exercise may be useful for ameliorating these adverse effects, although it is not completely effective. This review aimed to clarify how exercise interventions influenced body composition and bone mineral density and to explore the most effective exercise program among prostate cancer patients who received androgen deprivation therapy. We searched the PubMed, EMBASE, Web of Science, EBSCO, and Cochrane Library databases for reports of randomised controlled trials that were published until October 2021. All studies involved prostate cancer patients who received androgen deprivation therapy and completed aerobic exercise, resistance exercise, and/or impact exercise training. Outcomes were defined as lean body mass, body fat mass, body fat rate, regional and whole-body bone mineral density. Thirteen reports regarding 12 randomised clinical trials (715 participants) were included. Relative to the control group, exercise intervention provided a higher lean body mass (mean difference: 0.88, 95% confidence interval: 0.40 to 1.36, P<0.01), a lower body fat mass (mean difference: -0.60, 95% confidence interval: -1.10 to -0.10, P<0.05), and a lower body fat rate (mean difference: -0.93, 95% confidence interval: -1.39 to -0.47, P<0.01). Subgroup analyses revealed greater efficacy for exercise duration of ≥6 months (vs. <6 months) and exercise immediately after the therapy (vs. delayed exercise). No significant differences were observed in the bone mineral density outcomes. Exercise can help ameliorate the adverse effects of androgen deprivation therapy in body composition, with combination exercises including resistance exercise, 8-12 repetition maximum of resistance exercise intensity, prolonged exercise duration, and performing exercise immediately after therapy providing better amelioration. And the combination of resistance and impact exercise appears to be the best mode for improving the bone mineral density.
雄激素剥夺疗法是治疗前列腺癌的常用方法。然而,这种疗法会引起多种不良反应,如体脂增加和骨密度降低。运动可能有助于改善这些不良反应,但并非完全有效。本综述旨在阐明运动干预如何影响身体成分和骨密度,并探讨接受雄激素剥夺治疗的前列腺癌患者中最有效的运动方案。我们检索了 PubMed、EMBASE、Web of Science、EBSCO 和 Cochrane Library 数据库中截至 2021 年 10 月发表的随机对照试验报告。所有研究均纳入接受雄激素剥夺治疗并完成有氧运动、抗阻运动和/或冲击运动训练的前列腺癌患者。结局定义为瘦体重、体脂量、体脂率、局部和全身骨密度。纳入 13 项报告的 12 项随机临床试验(715 名参与者)。与对照组相比,运动干预提供了更高的瘦体重(均差:0.88,95%置信区间:0.40 至 1.36,P<0.01),更低的体脂量(均差:-0.60,95%置信区间:-1.10 至 -0.10,P<0.05)和更低的体脂率(均差:-0.93,95%置信区间:-1.39 至 -0.47,P<0.01)。亚组分析显示,运动持续时间≥6 个月(<6 个月)和治疗后立即运动(延迟运动)的效果更佳。骨密度结局无显著差异。运动可以帮助改善雄激素剥夺治疗对身体成分的不良影响,包括抗阻运动在内的组合运动、8-12 次重复最大抗阻运动强度、延长运动时间以及治疗后立即运动提供了更好的改善效果。抗阻和冲击运动的结合似乎是改善骨密度的最佳模式。