Asian Demographic Research Institute, Shanghai University, Shanghai, China.
International Institute for Applied Systems Analysis (IIASA), Wittgenstein Centre for Demography and Global Human Capital (IIASA, OeAW, University of Vienna), Laxenburg, Austria.
Front Public Health. 2022 Feb 11;10:749238. doi: 10.3389/fpubh.2022.749238. eCollection 2022.
Gender differences in mortality are embedded within mortality transitions. Rural residents generally lag behind their urban counterparts in the transitions. The study objective is to identify major causes of death that drive gender differences in mortality in urban and rural China.
We use age-, gender-, urban-rural- and cause-specific mortality data (2013-2018) derived from the national mortality surveillance system that covered about 24% of the Chinese population. We apply Arriaga's method to decompose age- and cause-specific contributions to the gender gap in life expectancy at birth. Analyses are stratified by urban-rural residence.
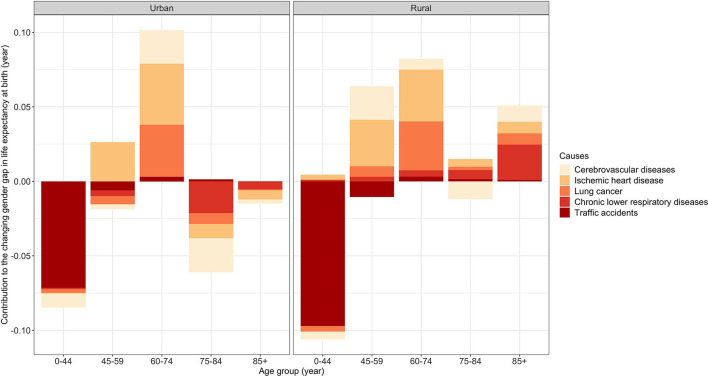
Women had a higher life expectancy at birth than men in both urban and rural areas. Cancers, cardiovascular disease, external causes, and respiratory disease accounted for more than 90% of the gender gap in both areas during 2013-2018. In urban areas, the gender gap decreased from 5.17 years in 2013-2015 to 4.98 years in 2016-2018. In rural areas, the gender gap stayed rather constant (2013-2015: 5.68 years; 2016-2018: 5.65 years). Traffic accidents, among external causes, contributed the most to decreasing the gender gap (urban: -0.07 years; rural: -0.10 years), especially in the 0-44 age group. However, the decrease in the gender gap was counteracted by an increase in the gender gap attributable to ischemic heart disease (urban: +0.05 years; rural: +0.08 years) and lung cancer (urban: +0.02 years; rural: +0.05 years) in older age groups. The gender gap attributable either to cerebrovascular disease or to chronic lower respiratory disease decreased in urban areas but increased in rural areas.
The urban-rural variations in the cause-specific contributions to the gender gap in China suggest the necessity of implementing urban-rural-specific interventions to improve population health and health equity.
性别死亡率差异存在于死亡率转变之中。农村居民的死亡率转变通常落后于城市居民。本研究旨在确定导致中国城乡两性死亡率差异的主要死因。
我们使用了全国死亡率监测系统中获得的年龄、性别、城乡和死因特异性死亡率数据(2013-2018 年),该系统覆盖了约 24%的中国人口。我们应用阿瑞亚加的方法,将年龄和死因特异性对出生时预期寿命性别差距的贡献进行分解。分析按照城乡居住情况进行分层。
在城乡地区,女性的出生时预期寿命均长于男性。2013-2018 年,癌症、心血管疾病、外部原因和呼吸道疾病占城乡两性差距的 90%以上。在城市地区,性别差距从 2013-2015 年的 5.17 岁缩小到 2016-2018 年的 4.98 岁。在农村地区,性别差距基本保持不变(2013-2015 年:5.68 岁;2016-2018 年:5.65 岁)。外部原因中的交通事故对缩小性别差距的贡献最大(城市:-0.07 岁;农村:-0.10 岁),尤其是 0-44 岁年龄组。然而,缺血性心脏病(城市:+0.05 岁;农村:+0.08 岁)和肺癌(城市:+0.02 岁;农村:+0.05 岁)在老年组中导致性别差距的增加,抵消了性别差距的缩小。城乡地区的脑血管病和慢性下呼吸道疾病导致的性别差距均有所缩小。
中国城乡性别死亡率差异的死因特异性贡献的差异表明,需要实施城乡特定的干预措施,以改善人口健康和健康公平。