Division of Rheumatology, Department of Medicine Solna, Karolinska Institutet and Karolinska University Hospital, Stockholm, Sweden.
Departments of Medicine and Rheumatology, The University of Melbourne at St Vincent's Hospital, Fitzroy.
Rheumatology (Oxford). 2022 Nov 28;61(12):4752-4762. doi: 10.1093/rheumatology/keac185.
To investigate the impact of remission and lupus low disease activity state (LLDAS) on health-related quality of life (HRQoL) in systemic lupus erythematosus.
Short-Form 36 (SF-36), three-level EQ-5D (EQ-5D-3L) and Functional Assessment of Chronic Illness Therapy (FACIT)-Fatigue data from the BLISS-52 (NCT00424476) and BLISS-76 (NCT00410384) trials were used. Duration in remission/LLDAS required to reach a HRQoL benefit ≥ minimal clinically important differences (MCIDs) during and post-treatment was determined using quantile regression and generalized estimating equations.
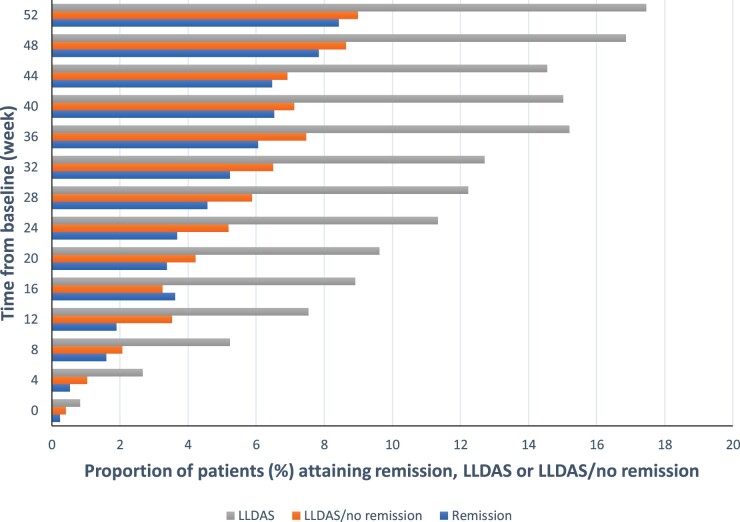
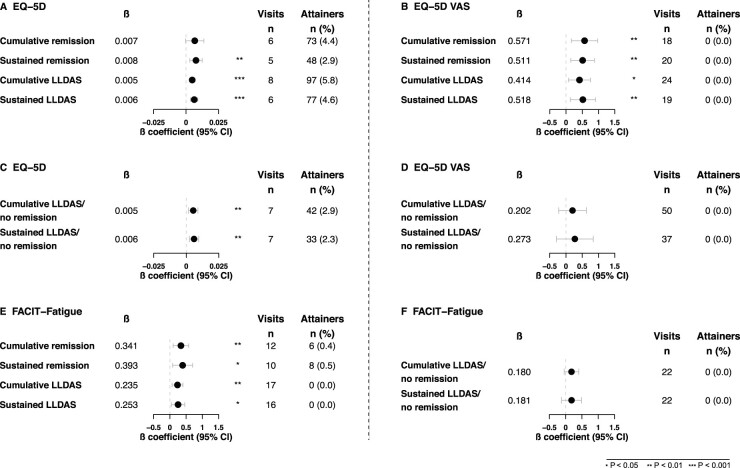
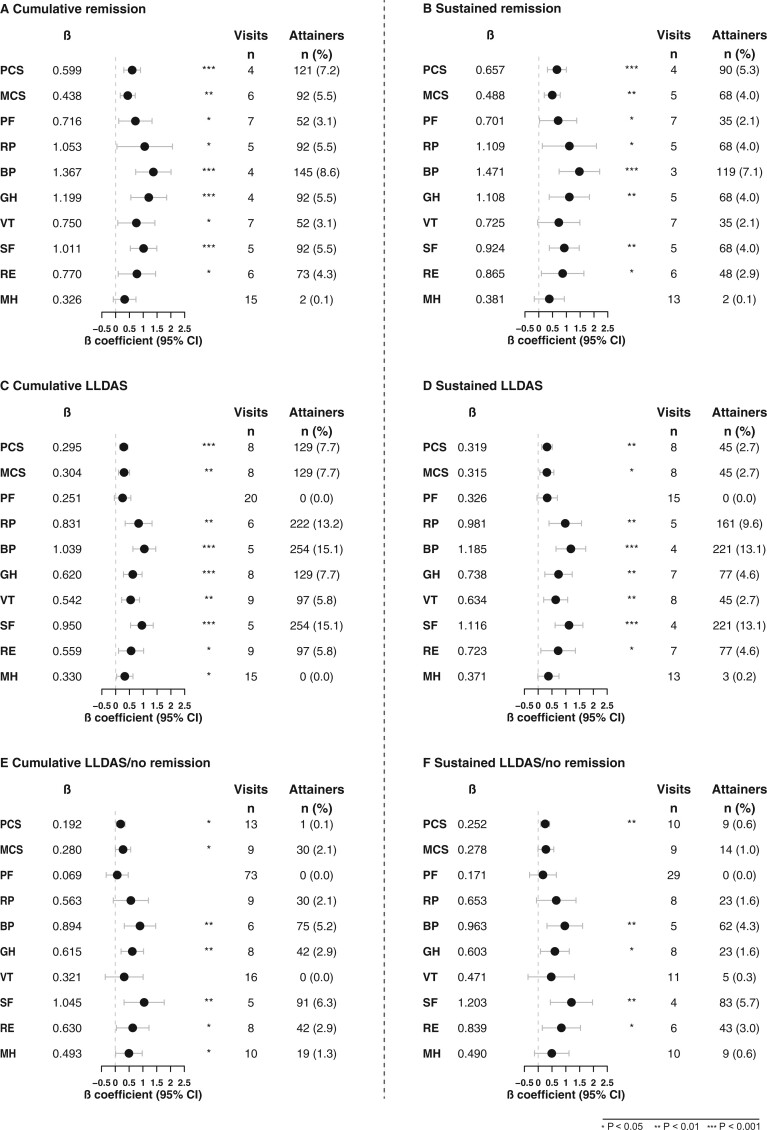
Patients (n = 1684) were assessed every fourth week (15 visits). Four cumulative (β = 0.60) or four consecutive (β = 0.66) visits in remission were required to achieve a benefit ≥MCID in SF-36 physical component summary (PCS) scores, and six cumulative (β = 0.44) or five consecutive (β = 0.49) for a benefit ≥MCID in mental component summary (MCS) scores. Eight cumulative (β = 0.30 for both) or eight consecutive (β = 0.32 for both) visits in LLDAS were required for a benefit in PCS/MCS ≥MCID, respectively. For EQ-5D-3L index scores ≥MCID, six cumulative (β = 0.007) or five consecutive (β = 0.008) visits in remission were required, and eight cumulative (β = 0.005) or six consecutive (β = 0.006) visits in LLDAS. For FACIT-Fatigue scores ≥MCID, 12 cumulative (β = 0.34) or 10 consecutive (β = 0.39) visits in remission were required, and 17 cumulative (β = 0.24) or 16 consecutive (β = 0.25) visits in LLDAS.
Remission and LLDAS contribute to a HRQoL benefit in a time-dependent manner. Shorter time in remission than in LLDAS was required for a clinically important benefit in HRQoL, and longer time in remission for a benefit in mental compared with physical HRQoL aspects. When remission/LLDAS was sustained, the same benefit was achieved in a shorter time.
探讨缓解和狼疮低疾病活动状态(LLDAS)对系统性红斑狼疮患者健康相关生活质量(HRQoL)的影响。
使用 BLISS-52(NCT00424476)和 BLISS-76(NCT00410384)试验中的短格式 36 项健康调查量表(SF-36)、三级 EQ-5D(EQ-5D-3L)和慢性病治疗功能评估量表-疲劳(FACIT-Fatigue)数据。采用分位数回归和广义估计方程确定达到治疗期间和治疗后 HRQoL 获益≥最小临床重要差异(MCID)所需的缓解/LLDAS 持续时间。
共评估了 1684 例患者(n=1684),每四周(15 次就诊)评估一次。需要 4 次连续(β=0.60)或 4 次累积(β=0.66)缓解期就诊才能使 SF-36 生理成分综合评分(PCS)获得≥MCID 的获益,需要 6 次连续(β=0.44)或 5 次连续(β=0.49)就诊才能使心理成分综合评分(MCS)获得≥MCID 的获益。需要 8 次连续(β=0.30,两者均为)或 8 次累积(β=0.32,两者均为)缓解期就诊才能使 PCS/MCS 获得≥MCID 的获益。需要 6 次连续(β=0.007)或 5 次连续(β=0.008)缓解期就诊才能使 EQ-5D-3L 指数评分获得≥MCID 的获益,需要 8 次连续(β=0.005)或 6 次连续(β=0.006)就诊才能使 LLDAS 获得≥MCID 的获益。需要 12 次连续(β=0.34)或 10 次连续(β=0.39)缓解期就诊才能使 FACIT-Fatigue 评分获得≥MCID 的获益,需要 17 次连续(β=0.24)或 16 次连续(β=0.25)就诊才能使 LLDAS 获得≥MCID 的获益。
缓解和 LLDAS 以时间依赖的方式有助于 HRQoL 的获益。与 LLDAS 相比,缓解期所需的时间更短,就能获得 HRQoL 的临床重要获益,且缓解期时间更长,可使心理 HRQoL 方面获益更大。当缓解/LLDAS 持续时,在更短的时间内获得相同的获益。