Key Laboratory of Carcinogenesis and Translational Research (Ministry of Education/Beijing), Department of Radiation Oncology, Peking University Cancer Hospital and Institute, Beijing, China.
Department of Radiation Oncology, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, China.
Br J Cancer. 2022 Jul;127(2):249-257. doi: 10.1038/s41416-022-01786-7. Epub 2022 Apr 2.
To analyse the performance of multicentre pre-treatment MRI-based radiomics (MBR) signatures combined with clinical baseline characteristics and neoadjuvant treatment modalities to predict complete response to neoadjuvant (chemo)radiotherapy in locally advanced rectal cancer (LARC).
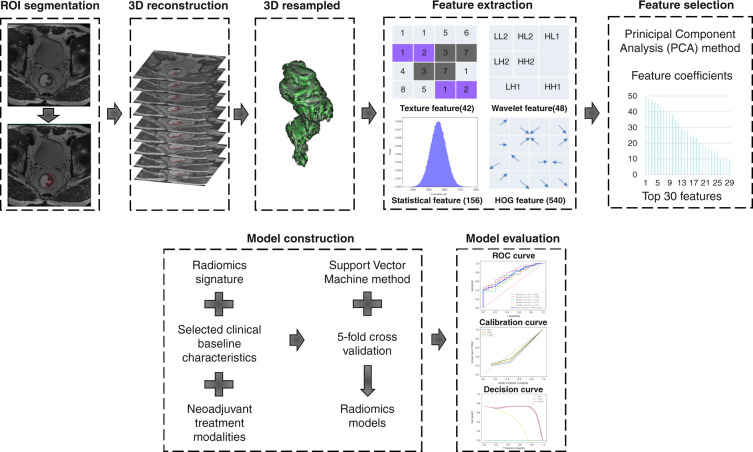
Baseline MRI and clinical characteristics with neoadjuvant treatment modalities at four centres were collected. Decision tree, support vector machine and five-fold cross-validation were applied for two non-imaging and three radiomics-based models' development and validation.
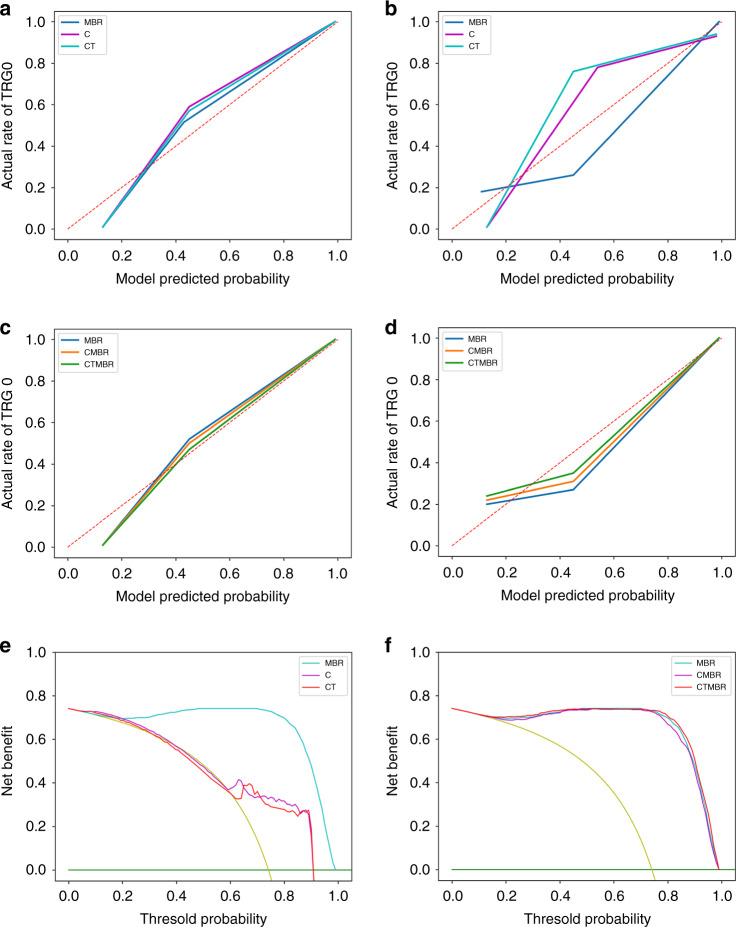
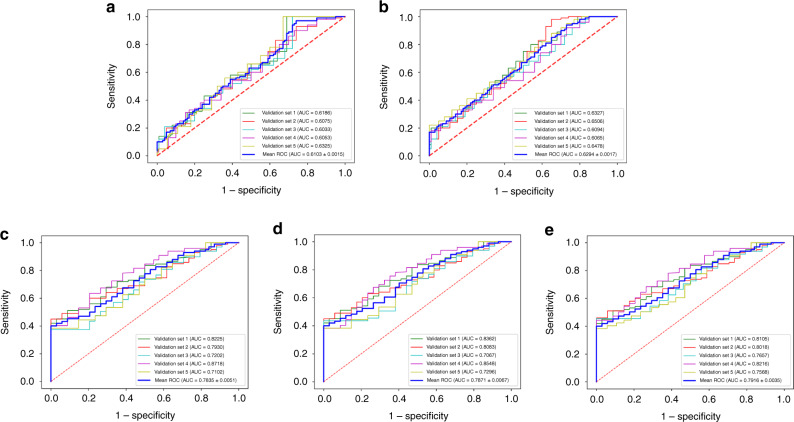
We finally included 674 patients. Pre-treatment CEA, T stage, and histologic grade were selected to generate two non-imaging models: C model (clinical baseline characteristics alone) and CT model (clinical baseline characteristics combining neoadjuvant treatment modalities). The prediction performance of both non-imaging models were poor. The MBR signatures comprising 30 selected radiomics features, the MBR signatures combining clinical baseline characteristics (CMBR), and the CMBR incorporating neoadjuvant treatment modalities (CTMBR) all showed good discrimination with mean AUCs of 0.7835, 0.7871 and 0.7916 in validation sets, respectively. The three radiomics-based models had insignificant discrimination in performance.
The performance of the radiomics-based models were superior to the non-imaging models. MBR signatures seemed to reflect LARC's true nature more accurately than clinical parameters and helped identify patients who can undergo organ preservation strategies.
分析多中心治疗前 MRI 特征(MBR)联合临床基线特征和新辅助治疗方法预测局部晚期直肠癌(LARC)新辅助(放)化疗完全缓解的性能。
在四个中心收集基线 MRI 和临床特征以及新辅助治疗方法。采用决策树、支持向量机和五折交叉验证方法开发和验证两个非影像和三个基于放射组学的模型。
我们最终纳入 674 例患者。治疗前 CEA、T 分期和组织学分级被选来生成两个非影像模型:C 模型(仅临床基线特征)和 CT 模型(临床基线特征结合新辅助治疗方法)。这两种非影像模型的预测性能都很差。包含 30 个选定放射组学特征的 MBR 特征、结合临床基线特征的 MBR 特征(CMBR)和纳入新辅助治疗方法的 CMBR(CTMBR),在验证组中的平均 AUC 分别为 0.7835、0.7871 和 0.7916,均显示出良好的区分度。三个基于放射组学的模型在性能上没有显著差异。
基于放射组学的模型的性能优于非影像模型。MBR 特征似乎比临床参数更能准确反映 LARC 的本质,有助于识别可以采用器官保存策略的患者。