Yao Wenjun, Yang Shuo, Ge Yaqiong, Fan Wenlong, Xiang Li, Wan Yang, Gu Kangchen, Zhao Yan, Zha Rujing, Bu Junjie
Department of Radiology, The Second Affiliated Hospital of Anhui Medical University, Hefei, China.
Department of Radiology, Anhui Mental Health Center, Hefei, China.
Front Med (Lausanne). 2022 Mar 24;9:819670. doi: 10.3389/fmed.2022.819670. eCollection 2022.
Due to the high recurrence rate in hepatocellular carcinoma (HCC) after resection, preoperative prognostic prediction of HCC is important for appropriate patient management. Exploring and developing preoperative diagnostic methods has great clinical value in treating patients with HCC. This study sought to develop and evaluate a novel combined clinical predictive model based on standard triphasic computed tomography (CT) to discriminate microvascular invasion (MVI) in hepatocellular carcinoma (HCC).
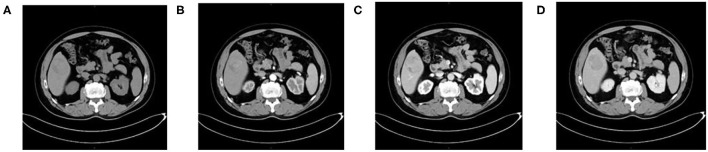
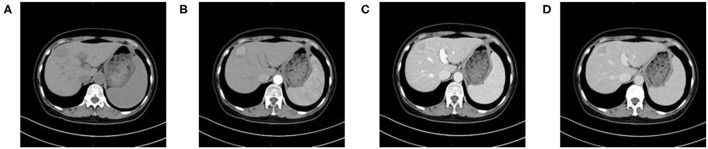
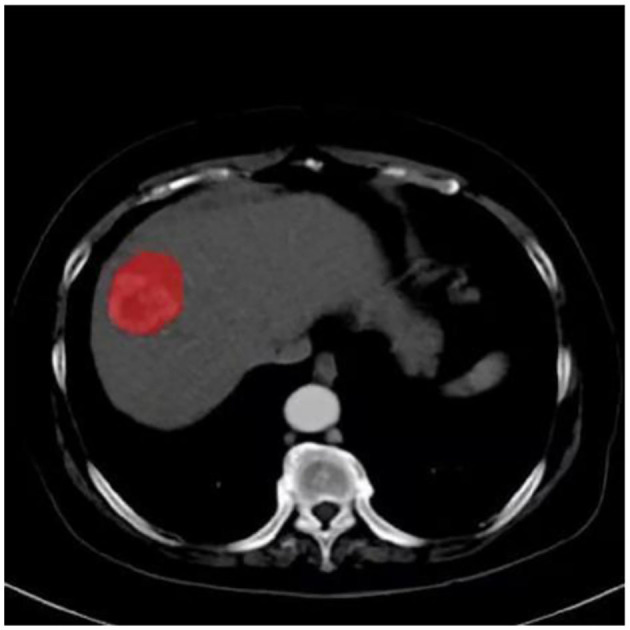
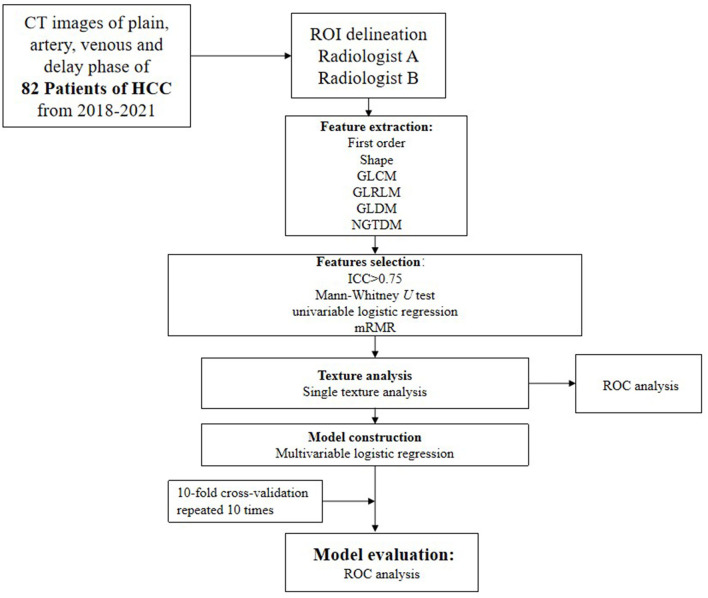
The preoperative findings of 82 patients with HCC, including conventional clinical factors, CT imaging findings, and CT texture analysis (TA), were analyzed retrospectively. All included cases were divided into MVI-negative ( = 33; no MVI) and MVI-positive ( = 49; low or high risk of MVI) groups. TA parameters were extracted from non-enhanced, arterial, portal venous, and equilibrium phase images and subsequently calculated using the Artificial Intelligence Kit. After statistical analyses, a clinical model comprising conventional clinical and CT image risk factors, radiomics signature models, and a novel combined model (fused radiomic signature) was constructed. The area under the curve (AUC) of the receiver operating characteristics (ROC) curve was used to assess the performance of the various models in discriminating MVI.
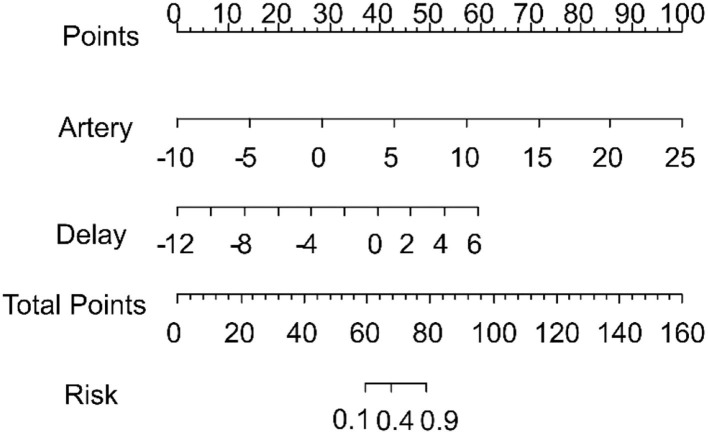
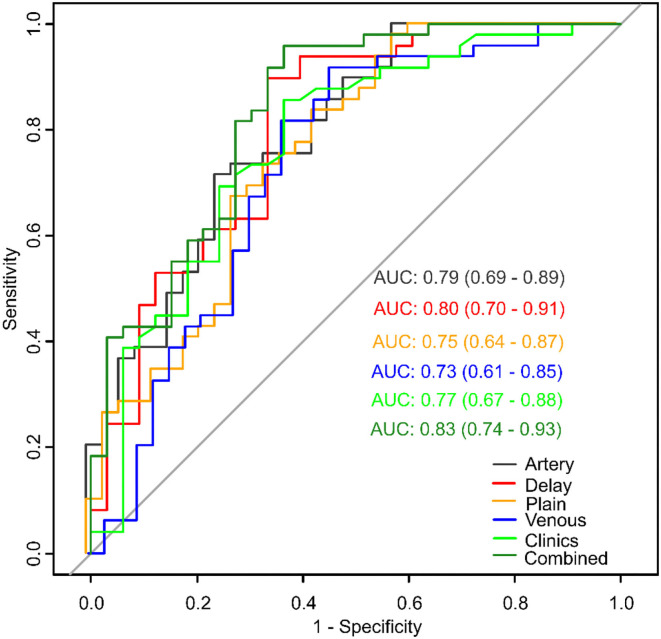
We found that tumor diameter and pathological grade were effective clinical predictors in clinical model and 12 radiomics features were effective for MVI prediction of each CT phase. The AUCs of the clinical, plain, artery, venous, and delay models were 0.77 (95% CI: 0.67-0.88), 0.75 (95% CI: 0.64-0.87), 0.79 (95% CI: 0.69-0.89), 0.73 (95% CI: 0.61-0.85), and 0.80 (95% CI: 0.70-0.91), respectively. The novel combined model exhibited the best performance, with an AUC of 0.83 (95% CI: 0.74-0.93).
Models derived from triphasic CT can preoperatively predict MVI in patients with HCC. Of the models tested here, the novel combined model was most predictive and could become a useful tool to guide subsequent personalized treatment of HCC.
由于肝细胞癌(HCC)切除术后复发率高,术前对HCC进行预后预测对于恰当的患者管理至关重要。探索和开发术前诊断方法在治疗HCC患者方面具有重要的临床价值。本研究旨在开发并评估一种基于标准三期计算机断层扫描(CT)的新型联合临床预测模型,以鉴别肝细胞癌(HCC)中的微血管侵犯(MVI)。
回顾性分析82例HCC患者的术前检查结果,包括传统临床因素、CT影像表现和CT纹理分析(TA)。所有纳入病例分为MVI阴性(n = 33;无MVI)和MVI阳性(n = 49;MVI低风险或高风险)组。从平扫、动脉期、门静脉期和平衡期图像中提取TA参数,随后使用人工智能套件进行计算。经过统计分析,构建了一个包含传统临床和CT影像危险因素的临床模型、影像组学特征模型以及一个新型联合模型(融合影像组学特征)。采用受试者操作特征(ROC)曲线下面积(AUC)评估各模型鉴别MVI的性能。
我们发现肿瘤直径和病理分级在临床模型中是有效的临床预测指标,并且12个影像组学特征对各CT期的MVI预测有效。临床模型、平扫模型、动脉期模型、门静脉期模型和延迟期模型的AUC分别为0.77(95%CI:0.67 - 0.88)、0.75(95%CI:0.64 - 0.87)、0.79(95%CI:0.69 - 0.89)、0.73(95%CI:0.61 - 0.85)和0.80(95%CI:0.70 - 0.91)。新型联合模型表现出最佳性能,AUC为0.83(95%CI:0.74 - 0.93)。
基于三期CT得出的模型可在术前预测HCC患者的MVI。在本研究测试的模型中,新型联合模型预测性最强,可成为指导后续HCC个体化治疗的有用工具。