Department of Anesthesia and Intensive Care, IRCCS San Raffaele Scientific Institute, Milan, Italy.
Department of Surgical Sciences and Integrated Diagnostic (DISC), University of Genoa, Viale Benedetto XV 6, Genoa, Italy.
Crit Care. 2022 May 6;26(1):126. doi: 10.1186/s13054-022-03993-3.
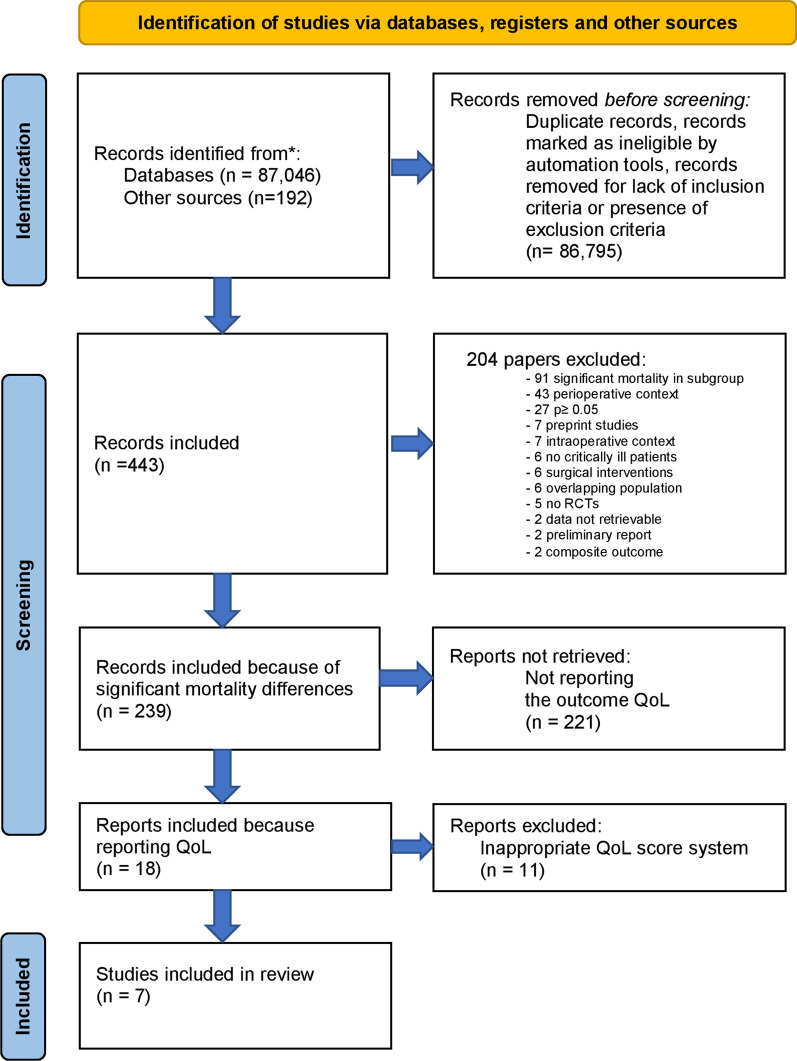
Survival has been considered the cornerstone for clinical outcome evaluation in critically ill patients admitted to intensive care unit (ICU). There is evidence that ICU survivors commonly show impairments in long-term outcomes such as quality of life (QoL) considering them as the most relevant ones. In the last years, the concept of patient-important outcomes has been introduced and increasingly reported in peer-reviewed publications. In the present systematic review, we evaluated how many randomized controlled trials (RCTs) were conducted on critically ill patients and reporting a benefit on survival reported also data on QoL. All RCTs investigating nonsurgical interventions that significantly reduced mortality in critically ill patients were searched on MEDLINE/PubMed, Scopus and Embase from inception until August 2021. In a second stage, for all the included studies, the outcome QoL was investigated. The primary outcome was to evaluate how many RCTs analyzing interventions reducing mortality reported also data on QoL. The secondary endpoint was to investigate if QoL resulted improved, worsened or not modified. Data on QoL were reported as evaluated outcome in 7 of the 239 studies (2.9%). The tools to evaluate QoL and QoL time points were heterogeneous. Four interventions showed a significant impact on QoL: Two interventions improved survival and QoL (pravastatin in subarachnoid hemorrhage, dexmedetomidine in elderly patients after noncardiac surgery), while two interventions reduced mortality but negatively influenced QoL (caloric restriction in patients with refeeding syndrome and systematic ICU admission in elderly patients). In conclusion, only a minority of RCTs in which an intervention demonstrated to affect mortality in critically ill patients reported also data on QoL. Future research in critical care should include patient-important outcomes like QoL besides mortality. Data on this topic should be collected in conformity with PROs statement and core outcome sets to guarantee quality and comparability of results.
生存一直被认为是评估重症监护病房(ICU)入住患者临床结局的基石。有证据表明,ICU 幸存者通常在长期结局方面存在损害,如生活质量(QoL),这被认为是最重要的结局。近年来,患者重要结局的概念已经被引入,并在同行评议的出版物中越来越多地被报道。在本系统评价中,我们评估了有多少针对危重病患者的随机对照试验(RCT)报告了生存获益,同时也报告了 QoL 数据。在 2021 年 8 月之前,我们在 MEDLINE/PubMed、Scopus 和 Embase 上搜索了所有关于非手术干预显著降低危重病患者死亡率的 RCT。在第二阶段,对所有纳入的研究,我们调查了 QoL 结局。主要结局是评估有多少分析降低死亡率的干预措施的 RCT 也报告了 QoL 数据。次要终点是调查 QoL 是否改善、恶化或未改变。在 239 项研究中的 7 项(2.9%)报告了 QoL 数据。评估 QoL 的工具和 QoL 时间点存在异质性。四项干预措施对 QoL 有显著影响:两项干预措施改善了生存和 QoL(蛛网膜下腔出血时的普伐他汀、老年非心脏手术后的右美托咪定),而两项干预措施降低了死亡率,但对 QoL 产生了负面影响(再喂养综合征患者的热量限制和老年患者的系统 ICU 入院)。总之,只有少数证明干预措施对危重病患者死亡率有影响的 RCT 报告了 QoL 数据。未来的重症监护研究应包括患者重要结局,如死亡率以外的 QoL。应根据 PROs 声明和核心结局集收集关于这一主题的数据,以保证结果的质量和可比性。