Medical School, Institute of Migration Health, University of Pécs, Pécs, Hungary.
Department of Anesthesiology and Intensive Care, Medical School, University of Pécs, Pécs, Hungary.
Front Endocrinol (Lausanne). 2022 May 6;13:870465. doi: 10.3389/fendo.2022.870465. eCollection 2022.
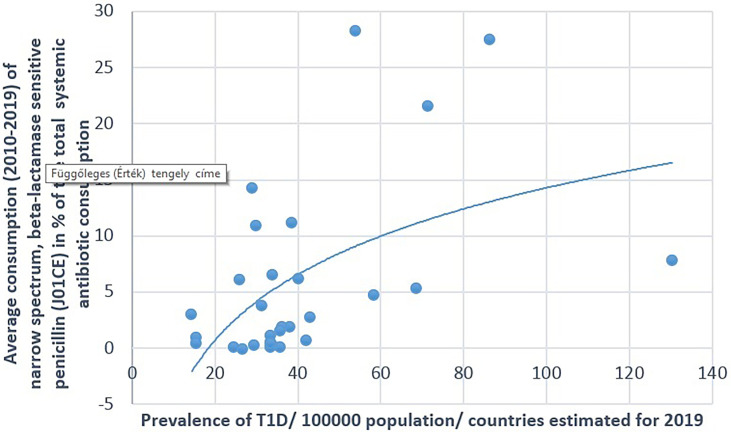
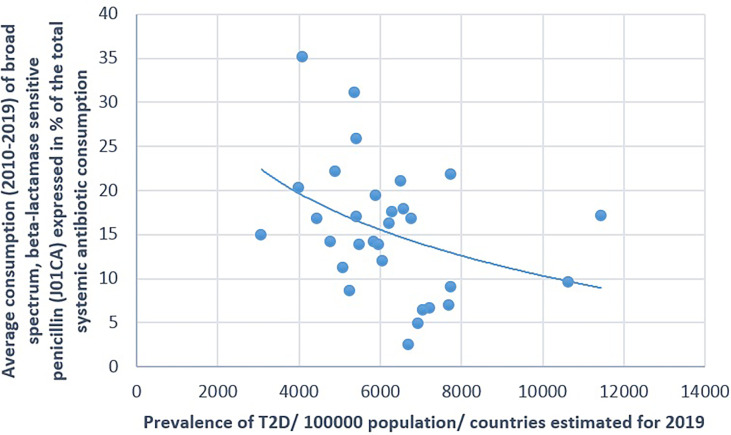
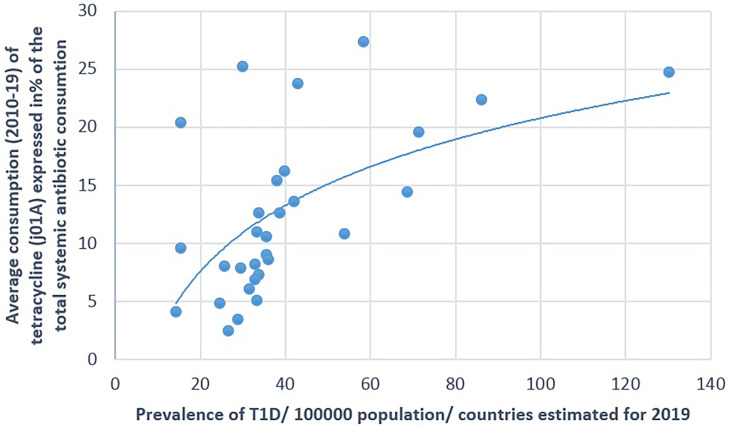
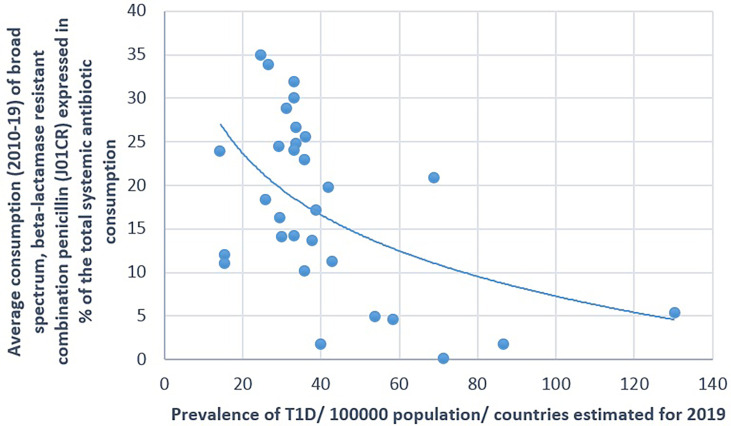
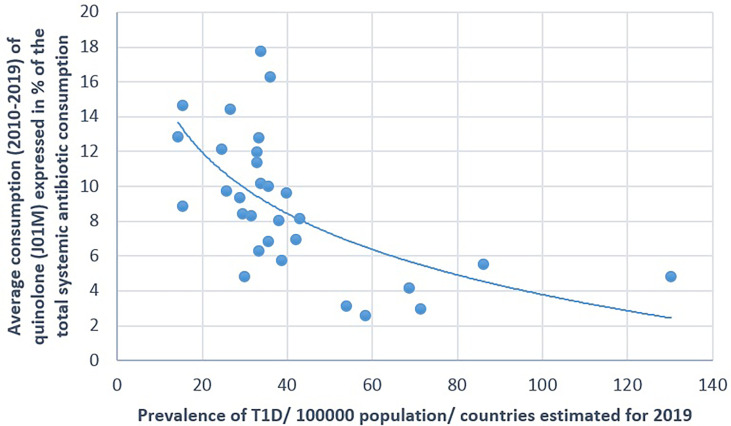
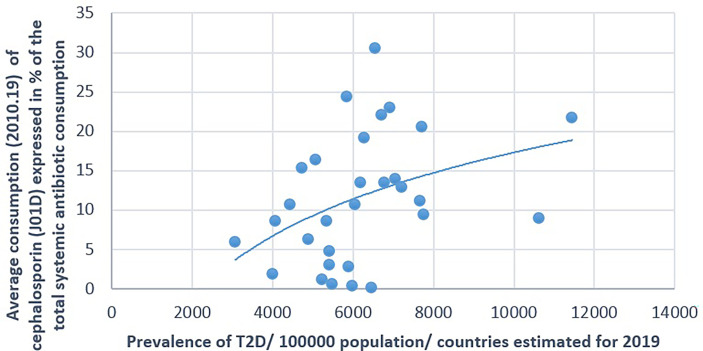
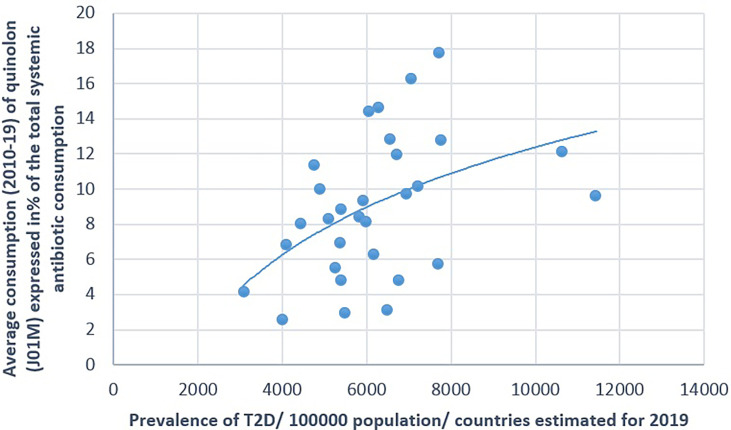
Several publications have raised the issue that the development of diabetes precedes the alteration of the microbiome (dysbiosis) and the role of environmental factors. Antibiotic use induces dysbiosis, and we wanted to estimate the associations between the consumption of antibiotics and the prevalence of diabetes (both types 1 and 2; T1D and T2D, respectively) in European countries. If such an association exists, the dominant use antibiotic classes might be reflected in the prevalence rates of T1D and T2D in different countries. Comparisons were performed between the prevalence of diabetes estimated for 2019 and featured in the Diabetes Atlas and the average yearly consumption of antibiotic classes between 2010 and 2109, calculated from the European Centre for Disease Prevention and Control (ECDC) yearly reports on antibiotic consumption in Europe. Pearson's correlation and variance analyses were used to estimate the possible relationship. Strong positive (enhancer) associations were found between the prevalence of T1D and the consumption of tetracycline (J01A: = 0.001) and the narrow-spectrum penicillin (J01CE: = 0.006; CF: = 0.018). A strong negative (inhibitor) association was observed with broad-spectrum, beta-lactamase-resistant penicillin (J01CR: = 0.003), macrolide (J01F: = 0.008), and quinolone (J01M: = 0.001). T2D showed significant positive associations with cephalosporin (J01D: = 0.048) and quinolone (J01M: = 0.025), and a non-significant negative association was detected with broad-spectrum, beta-lactamase-sensitive penicillin (J01CA: = 0.067). Countries showing the highest prevalence rates of diabetes (top 10) showed concordance with the higher consumption of "enhancer" and the lower consumption of "inhibitor" antibiotics (top 10), as indicated by variance analysis. Countries with high prevalence rates of T1D showed high consumption of tetracycline ( = 0.015) and narrow-spectrum, beta-lactamase sensitive penicillin ( = 0.008) and low consumption of "inhibitor" antibiotics [broad-spectrum, beta-lactamase-resistant, combination penicillin ( = 0.005); cephalosporin ( = 0.036); and quinolone ( = 0.003)]. Countries with high prevalence rates of T2D consumed more cephalosporin ( = 0.084) and quinolone ( = 0.054) and less broad-spectrum, beta-lactamase-sensitive penicillin ( = 0.012) than did other countries. The development of diabetes-related dysbiosis might be related to the higher consumption of specific classes of antibiotics, showing positive (enhancer) associations with the prevalence of diabetes, and the low consumption of other classes of antibiotics, those showing negative (inhibitory) associations. These groups of antibiotics are different in T1D and T2D.
已有多项出版物提出,糖尿病的发展先于微生物组(失调)的改变,且环境因素也起着一定作用。抗生素的使用会导致失调,我们希望评估欧洲国家抗生素的使用与糖尿病(包括 1 型和 2 型糖尿病;T1D 和 T2D)的流行之间的相关性。如果存在这种相关性,那么不同国家 T1D 和 T2D 的流行率可能反映出主要使用的抗生素类别。我们将 2019 年《糖尿病地图集》中估计的糖尿病流行率与 2010 年至 2019 年欧洲疾病预防控制中心(ECDC)每年报告的抗生素消费数据进行了比较,抗生素消费数据是按类别计算的。采用 Pearson 相关和方差分析来估计可能的关系。我们发现 T1D 的流行率与四环素(J01A: = 0.001)和窄谱青霉素(J01CE: = 0.006;CF: = 0.018)的消费之间存在强烈的正相关(增强剂)关系。广谱、耐β-内酰胺酶青霉素(J01CR: = 0.003)、大环内酯类(J01F: = 0.008)和喹诺酮类(J01M: = 0.001)的消费与 T1D 呈显著负相关(抑制剂)。T2D 与头孢菌素(J01D: = 0.048)和喹诺酮类(J01M: = 0.025)呈显著正相关,与广谱、β-内酰胺酶敏感青霉素(J01CA: = 0.067)呈非显著负相关。糖尿病流行率最高的(前 10 位)国家与抗生素“增强剂”的高消费和“抑制剂”的低消费相一致(前 10 位),这一点通过方差分析得到了证实。T1D 流行率较高的国家抗生素消费较高,包括四环素( = 0.015)和窄谱、β-内酰胺酶敏感青霉素( = 0.008),以及“抑制剂”抗生素的消费较低[广谱、β-内酰胺酶耐药、组合青霉素( = 0.005);头孢菌素( = 0.036);和喹诺酮类( = 0.003)]。T2D 流行率较高的国家头孢菌素( = 0.084)和喹诺酮类( = 0.054)的消费较高,而广谱、β-内酰胺酶敏感青霉素( = 0.012)的消费较低。与其他国家相比,这些国家的 T1D 和 T2D 相关的糖尿病相关失调的发展可能与特定类别的抗生素消费较高有关,这些抗生素与糖尿病的流行呈正相关(增强剂),而其他类别的抗生素消费较低,呈负相关(抑制剂)。这些抗生素类别在 T1D 和 T2D 中有所不同。