Department of Internal Medicine, Endocrinology and Metabolism, Azienda Ospedaliera Santa Maria Misericordia, Ospedale di Perugia, Piazzale Gambuli, 06081 Perugia, Italy.
Department of Pharmaceutical Sciences, Human Anatomy Laboratory, University of Perugia, 06132 Perugia, Italy.
Int J Mol Sci. 2022 May 14;23(10):5511. doi: 10.3390/ijms23105511.
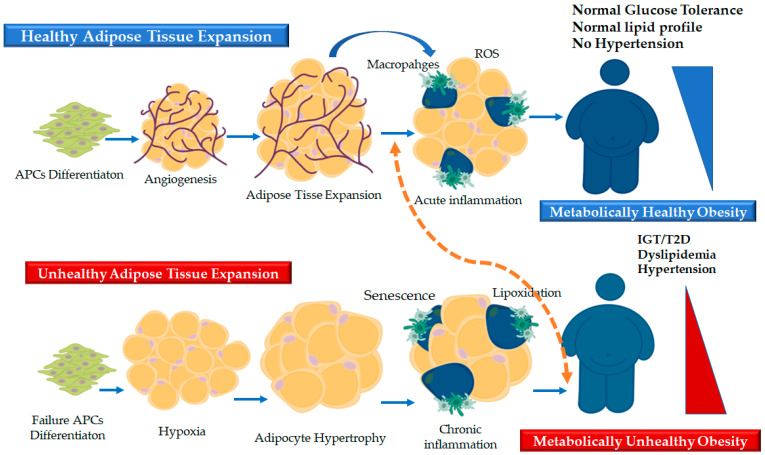
Adipose tissue (AT) is a remarkably plastic and active organ with functional pleiotropism and high remodeling capacity. Although the expansion of fat mass, by definition, represents the hallmark of obesity, the dysregulation of the adipose organ emerges as the forefront of the link between adiposity and its associated metabolic and cardiovascular complications. The dysfunctional fat displays distinct biological signatures, which include enlarged fat cells, low-grade inflammation, impaired redox homeostasis, and cellular senescence. While these events are orchestrated in a cell-type, context-dependent and temporal manner, the failure of the adipose precursor cells to form new adipocytes appears to be the main instigator of the adipose dysregulation, which, ultimately, poses a deleterious milieu either by promoting ectopic lipid overspill in non-adipose targets (i.e., lipotoxicity) or by inducing an altered secretion of different adipose-derived hormones (i.e., adipokines and lipokines). This "adipocentric view" extends the previous "expandability hypothesis", which implies a reduced plasticity of the adipose organ at the nexus between unhealthy fat expansion and the development of obesity-associated comorbidities. In this review, we will briefly summarize the potential mechanisms by which adaptive changes to variations of energy balance may impair adipose plasticity and promote fat organ dysfunction. We will also highlight the conundrum with the perturbation of the adipose microenvironment and the development of cardio-metabolic complications by focusing on adipose lipoxidation, inflammation and cellular senescence as a novel triad orchestrating the conspiracy to adipose dysfunction. Finally, we discuss the scientific rationale for proposing adipose organ plasticity as a target to curb/prevent adiposity-linked cardio-metabolic complications.
脂肪组织(AT)是一种具有显著可塑性和多功能性的活跃器官,具有功能多样性和高重塑能力。尽管脂肪量的扩张,根据定义,代表肥胖的标志,但脂肪器官的失调作为肥胖及其相关代谢和心血管并发症之间联系的前沿出现。功能失调的脂肪表现出明显的生物学特征,包括脂肪细胞增大、低度炎症、氧化还原平衡受损和细胞衰老。虽然这些事件以细胞类型、上下文依赖和时间依赖的方式进行协调,但脂肪前体细胞形成新脂肪细胞的失败似乎是脂肪失调的主要引发因素,最终通过促进非脂肪组织中异位脂质溢出(即脂毒性)或通过诱导不同脂肪衍生激素(即脂肪因子和脂联素)的改变分泌来产生有害环境。这种“脂肪中心观点”扩展了以前的“可扩展性假说”,该假说暗示不健康脂肪扩张和肥胖相关并发症发展之间的脂肪器官可塑性降低。在这篇综述中,我们将简要总结能量平衡变化适应变化可能损害脂肪可塑性并促进脂肪器官功能障碍的潜在机制。我们还将重点关注脂肪氧化、炎症和细胞衰老作为协调脂肪功能障碍阴谋的新三联体,强调脂肪微环境的扰动和心脏代谢并发症的发展的难题。最后,我们讨论了将脂肪器官可塑性作为抑制/预防与肥胖相关的心脏代谢并发症的目标的科学依据。