Department of Orthopaedic Surgery and Traumatology, HFR Hôpital Cantonal, University of Fribourg, 1700 Fribourg, Switzerland.
Department of Orthopaedic Surgery and Traumatology, Kantonsspital Aarau AG, 5001 Aarau, Switzerland.
Medicina (Kaunas). 2022 Jun 20;58(6):832. doi: 10.3390/medicina58060832.
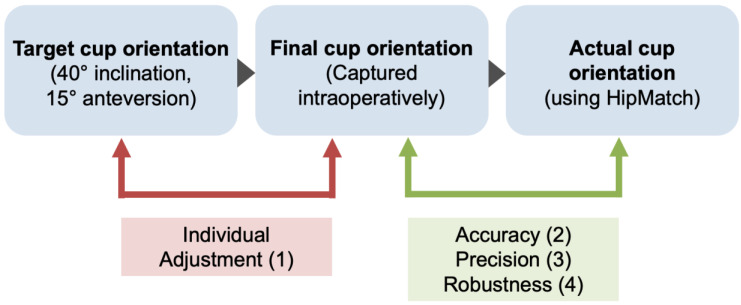
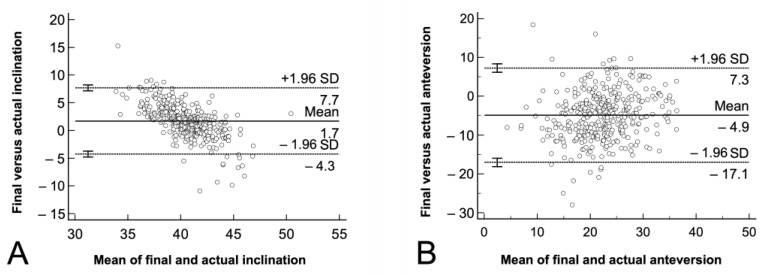
Background and Objectives: Even after the ‘death’ of Lewinnek’s safe zone, the orientation of the prosthetic cup in total hip arthroplasty is crucial for success. Accurate cup placement can be achieved with surgical navigation systems. The literature lacks study cohorts with large numbers of hips because postoperative computer tomography is required for the reproducible evaluation of the acetabular component position. To overcome this limitation, we used a validated software program, HipMatch, to accurately assess the cup orientation based on an anterior-posterior pelvic X-ray. The aim of this study were to (1) determine the intraoperative ‘individual adjustment’ of the cup positioning compared to the widely suggested target values of 40° of inclination and 15° of anteversion, and evaluate the (2) ‘accuracy’, (3) ‘precision’, and (4) robustness, regarding systematic errors, of an image-free navigation system in routine clinical use. Material and Methods: We performed a retrospective, accuracy study in a single surgeon case series of 367 navigated primary total hip arthroplasties (PiGalileoTM, Smith+Nephew) through an anterolateral approach performed between January 2011 and August 2018. The individual adjustments were defined as the differences between the target cup orientation (40° of inclination, 15° of anteversion) and the intraoperative registration with the navigation software. The accuracy was the difference between the intraoperative captured cup orientation and the actual postoperative cup orientation determined by HipMatch. The precision was analyzed by the standard deviation of the difference between the intraoperative registered and the actual cup orientation. The outliers were detected using the Tukey method. Results: Compared to the target value (40° inclination, 15° anteversion), the individual adjustments showed that the cups are impacted in higher inclination (mean 3.2° ± 1.6°, range, (−2)−18°) and higher anteversion (mean 5.0° ± 7.0°, range, (−15)−23°) (p < 0.001). The accuracy of the navigated cup placement was −1.7° ± 3.0°, ((−15)−11°) for inclination, and −4.9° ± 6.2° ((−28)−18°) for anteversion (p < 0.001). Precision of the system was higher for inclination (standard deviation SD 3.0°) compared to anteversion (SD 6.2°) (p < 0.001). We found no difference in the prevalence of outliers for inclination (1.9% (7 out of 367)) compared to anteversion (1.63% (6 out of 367), p = 0.78). The Bland-Altman analysis showed that the differences between the intraoperatively captured final position and the postoperatively determined actual position were spread evenly and randomly for inclination and anteversion. Conclusion: The evaluation of an image-less navigation system in this large study cohort provides accurate and reliable intraoperative feedback. The accuracy and the precision were inferior compared to CT-based navigation systems particularly regarding the anteversion. However the assessed values are certainly within a clinically acceptable range. This use of image-less navigation offers an additional tool to address challenging hip prothesis in the context of the hip−spine relationship to achieve adequate placement of the acetabular components with a minimum of outliers.
即使在 Lewinnek 安全区“死亡”后,全髋关节置换术中假体杯的方向对于手术的成功仍然至关重要。手术导航系统可以实现准确的杯位放置。由于需要术后计算机断层扫描(CT)来对髋臼部件位置进行可重复的评估,因此文献中缺乏大量髋关节的研究队列。为了克服这一限制,我们使用了经过验证的软件程序 HipMatch,根据前后骨盆 X 射线准确评估杯的方向。本研究的目的是:(1)与广泛建议的 40°倾斜和 15°前倾角的目标值相比,确定术中杯定位的“个体调整”,并评估(2)无图像导航系统在常规临床使用中的“准确性”、(3)“精密度”和(4)“稳健性”,包括系统误差。 材料与方法:我们进行了一项回顾性、准确性研究,纳入了 2011 年 1 月至 2018 年 8 月间由同一位外科医生通过前外侧入路进行的 367 例导航初次全髋关节置换术(PiGalileoTM,Smith+Nephew)的单外科医生病例系列。个体调整定义为目标杯方向(40°倾斜,15°前倾角)与术中与导航软件注册之间的差异。准确性是术中捕获的杯位置与 HipMatch 确定的实际术后杯位置之间的差异。精度通过术中注册和实际杯位置之间的差异的标准差进行分析。使用 Tukey 方法检测离群值。 结果:与目标值(40°倾斜,15°前倾角)相比,个体调整显示杯的倾斜度更高(平均 3.2°±1.6°,范围(-2)-18°),前倾角更高(平均 5.0°±7.0°,范围(-15)-23°)(p<0.001)。导航杯放置的准确性为-1.7°±3.0°,(-15)-11°)用于倾斜度,-4.9°±6.2°(-28)-18°)用于前倾角(p<0.001)。系统的精度对于倾斜度较高(标准偏差 SD 3.0°),而前倾角(SD 6.2°)较低(p<0.001)。我们发现倾斜度的离群值发生率(1.9%(7/367))与前倾角(1.63%(6/367))无差异(p=0.78)。Bland-Altman 分析表明,术中捕获的最终位置和术后确定的实际位置之间的差异在倾斜度和前倾角上均匀且随机分布。 结论:在这项大型研究队列中对无图像导航系统的评估提供了准确可靠的术中反馈。准确性和精密度与基于 CT 的导航系统相比有所下降,特别是在涉及前倾角时。然而,评估值肯定在临床可接受的范围内。这种无图像导航的使用提供了一种额外的工具,可以在髋关节-脊柱关系的背景下解决具有挑战性的髋关节假体,以实现髋臼部件的适当放置,并且离群值的数量最少。