Koehler Felix C, Di Cristanziano Veronica, Späth Martin R, Hoyer-Allo K Johanna R, Wanken Manuel, Müller Roman-Ulrich, Burst Volker
Department II of Internal Medicine and Center for Molecular Medicine Cologne, University of Cologne, Faculty of Medicine and University Hospital Cologne, Cologne, Germany.
Institute of Virology, University of Cologne, Faculty of Medicine and University Hospital of Cologne, Cologne, Germany.
Clin Kidney J. 2022 Jan 29;15(7):1231-1252. doi: 10.1093/ckj/sfac008. eCollection 2022 Jul.
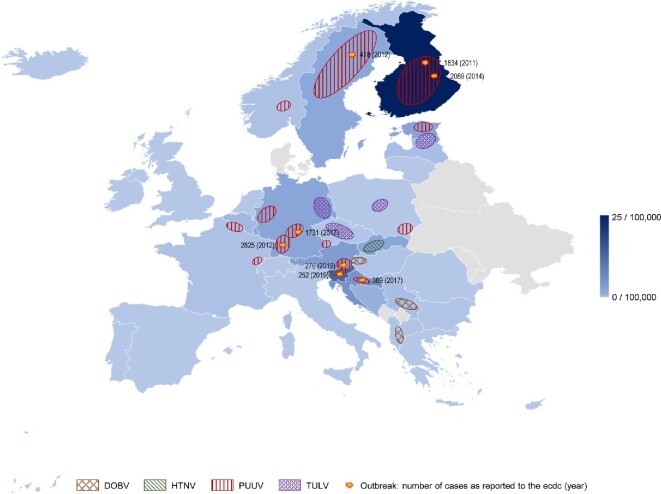
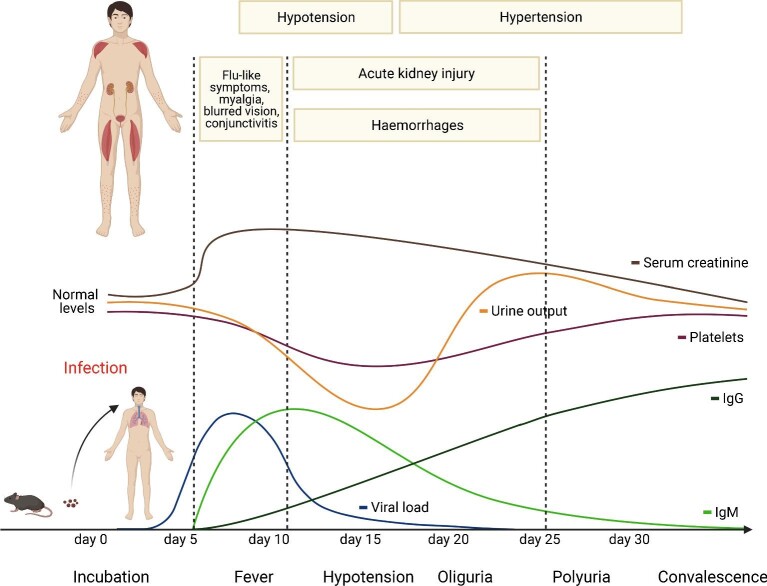
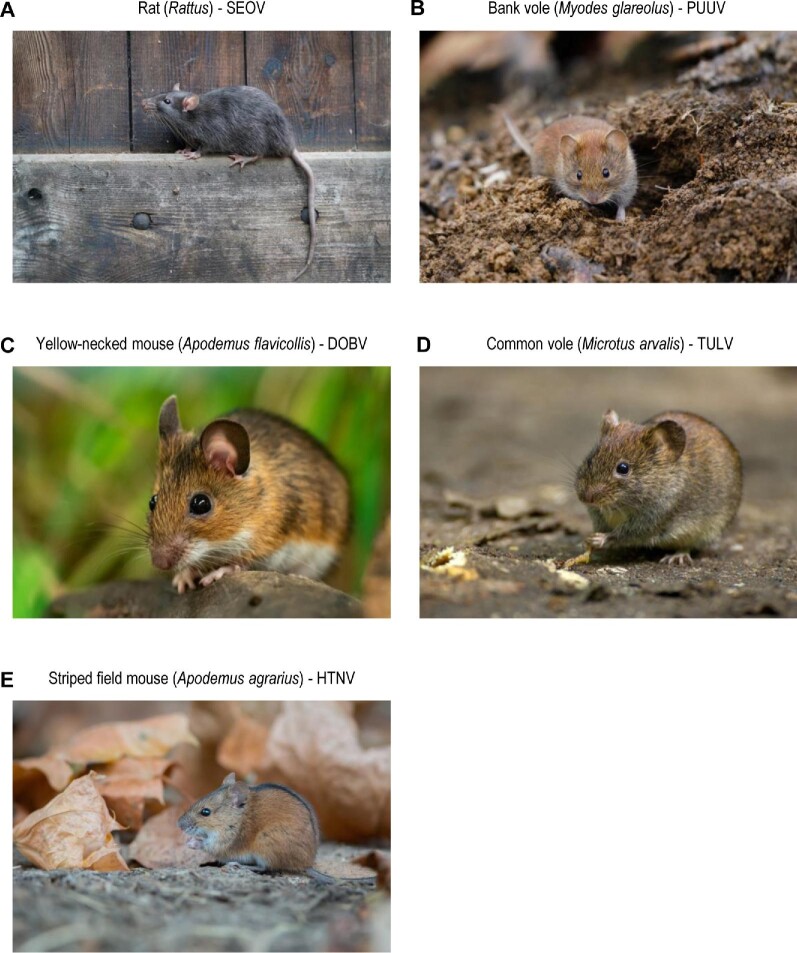
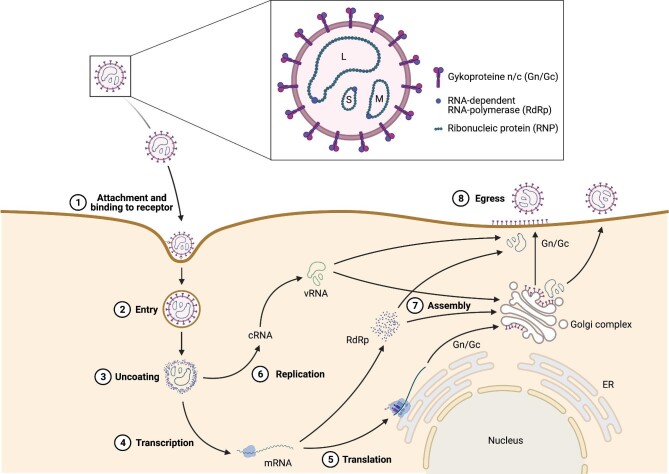
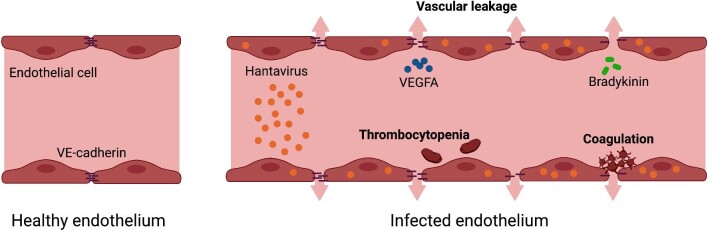
Hantavirus-induced diseases are emerging zoonoses with endemic appearances and frequent outbreaks in different parts of the world. In humans, hantaviral pathology is characterized by the disruption of the endothelial cell barrier followed by increased capillary permeability, thrombocytopenia due to platelet activation/depletion and an overactive immune response. Genetic vulnerability due to certain human leukocyte antigen haplotypes is associated with disease severity. Typically, two different hantavirus-caused clinical syndromes have been reported: hemorrhagic fever with renal syndrome (HFRS) and hantavirus cardiopulmonary syndrome (HCPS). The primarily affected vascular beds differ in these two entities: renal medullary capillaries in HFRS caused by Old World hantaviruses and pulmonary capillaries in HCPS caused by New World hantaviruses. Disease severity in HFRS ranges from mild, e.g. Puumala virus-associated nephropathia epidemica, to moderate, e.g. Hantaan or Dobrava virus infections. HCPS leads to a severe acute respiratory distress syndrome with high mortality rates. Due to novel insights into organ tropism, hantavirus-associated pathophysiology and overlapping clinical features, HFRS and HCPS are believed to be interconnected syndromes frequently involving the kidneys. As there are no specific antiviral treatments or vaccines approved in Europe or the USA, only preventive measures and public awareness may minimize the risk of hantavirus infection. Treatment remains primarily supportive and, depending on disease severity, more invasive measures (e.g., renal replacement therapy, mechanical ventilation and extracorporeal membrane oxygenation) are needed.
汉坦病毒引起的疾病是一种新发人兽共患病,在世界不同地区呈地方性流行且频繁暴发。在人类中,汉坦病毒病理学特征为内皮细胞屏障破坏,随后毛细血管通透性增加、因血小板激活/耗竭导致血小板减少以及免疫反应过度活跃。某些人类白细胞抗原单倍型导致的遗传易感性与疾病严重程度相关。通常,已报道两种由汉坦病毒引起的不同临床综合征:肾综合征出血热(HFRS)和汉坦病毒肺综合征(HCPS)。这两种疾病主要累及的血管床不同:旧世界汉坦病毒引起的HFRS累及肾髓质毛细血管,新世界汉坦病毒引起的HCPS累及肺毛细血管。HFRS的疾病严重程度范围从轻度,如普马拉病毒相关的流行性肾病,到中度,如汉坦病毒或多布拉伐病毒感染。HCPS会导致严重的急性呼吸窘迫综合征,死亡率很高。由于对病毒嗜性、汉坦病毒相关病理生理学以及重叠临床特征有了新的认识,HFRS和HCPS被认为是经常累及肾脏的相互关联的综合征。由于在欧洲或美国没有批准的特异性抗病毒治疗方法或疫苗,只有预防措施和公众意识可以将汉坦病毒感染风险降至最低。治疗仍以支持性治疗为主,根据疾病严重程度,需要采取更具侵入性的措施(如肾脏替代治疗、机械通气和体外膜肺氧合)。