Faculty of Medicine and Health, The University of Sydney, Sydney School of Public Health, Menzies Centre for Health Policy and Economics, Sydney, New South Wales, Australia.
School of Health and Rehabilitation Sciences, The University of Queensland, Brisbane, Queensland, Australia.
Pain Med. 2022 Dec 1;23(12):1979-2009. doi: 10.1093/pm/pnac102.
This scoping review aimed to comprehensively review strategies for implementation of low back pain (LBP) guidelines, policies, and models of care in the Australian health care system.
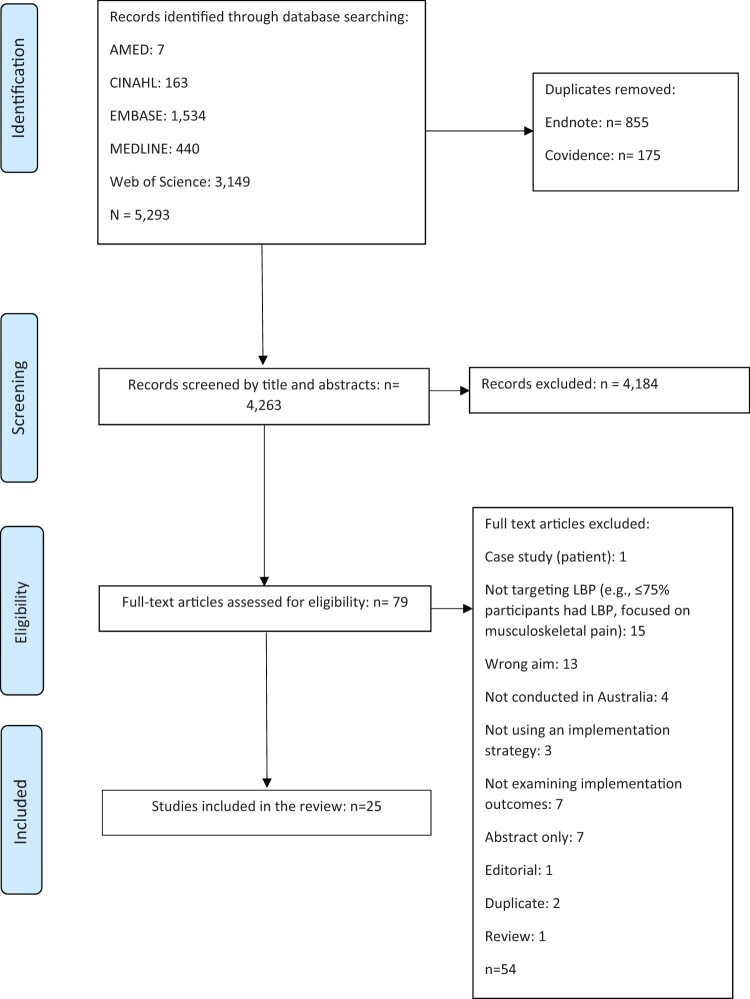
A literature search was conducted in MEDLINE, EMBASE, CINAHL, Allied and Complementary Medicine Database, and Web of Science to identify studies that aimed to implement or integrate evidence-based interventions or practices to improve LBP care within Australian settings.
Twenty-five studies met the inclusion criteria. Most studies targeted primary care settings (n = 13). Other settings included tertiary care (n = 4), community (n = 4), and pharmacies (n = 3). One study targeted both primary and tertiary care settings (n = 1). Only 40% of the included studies reported an underpinning framework, model, or theory. The implementation strategies most frequently used were evaluative and iterative strategies (n = 14, 56%) and train and educate stakeholders (n = 13, 52%), followed by engage consumers (n = 6, 24%), develop stakeholder relationships (n = 4, 16%), change in infrastructure (n = 4, 16%), and support clinicians (n = 3, 12%). The most common implementation outcomes considered were acceptability (n = 11, 44%) and adoption (n = 10, 40%), followed by appropriateness (n = 7, 28%), cost (n = 3, 12%), feasibility (n = 1, 4%), and fidelity (n = 1, 4%). Barriers included time constraints, funding, and teamwork availability. Facilitators included funding and collaboration between stakeholders.
Implementation research targeting LBP appears to be a young field, mostly focusing on training and educating stakeholders in primary care. Outcomes on sustainability and penetration of evidence-based interventions are lacking. There is a need for implementation research guided by established frameworks that consider interrelationships between organizational and system contexts beyond the clinician-patient dyad.
本范围综述旨在全面审查在澳大利亚医疗保健系统中实施腰痛 (LBP) 指南、政策和护理模式的策略。
在 MEDLINE、EMBASE、CINAHL、补充和综合医学数据库以及 Web of Science 中进行文献检索,以确定旨在实施或整合循证干预或实践以改善澳大利亚环境中 LBP 护理的研究。
25 项研究符合纳入标准。大多数研究针对初级保健环境(n=13)。其他环境包括三级保健(n=4)、社区(n=4)和药店(n=3)。一项研究针对初级和三级保健环境(n=1)。仅 40%的纳入研究报告了基础框架、模型或理论。最常使用的实施策略是评估和迭代策略(n=14,56%)和培训和教育利益相关者(n=13,52%),其次是让消费者参与(n=6,24%)、建立利益相关者关系(n=4,16%)、改变基础设施(n=4,16%)和支持临床医生(n=3,12%)。考虑的最常见实施结果是可接受性(n=11,44%)和采用(n=10,40%),其次是适宜性(n=7,28%)、成本(n=3,12%)、可行性(n=1,4%)和保真度(n=1,4%)。障碍包括时间限制、资金和团队合作可用性。促进因素包括资金和利益相关者之间的合作。
针对 LBP 的实施研究似乎是一个年轻的领域,主要集中在初级保健中培训和教育利益相关者。缺乏关于可持续性和循证干预措施渗透的结果。需要有循证框架指导的实施研究,该框架考虑到组织和系统背景之间的相互关系,超出临床医生-患者对子。