Ding Jie, Zhang Ying, Amjad Asma, Xu Jiaofeng, Thill Daniel, Li X Allen
Department of Radiation Oncology, Medical College of Wisconsin, Milwaukee, Wisconsin.
Elekta Inc, St. Charles, Missouri.
Adv Radiat Oncol. 2022 Apr 20;7(5):100968. doi: 10.1016/j.adro.2022.100968. eCollection 2022 Sep-Oct.
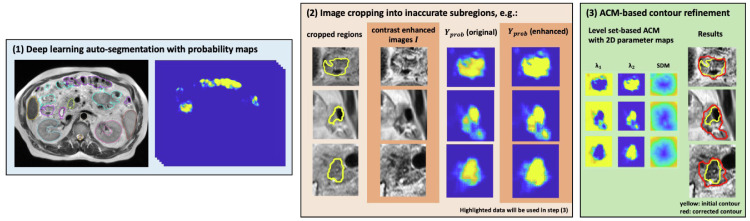
Fast and accurate auto-segmentation on daily images is essential for magnetic resonance imaging (MRI)-guided adaptive radiation therapy (ART). However, the state-of-the-art auto-segmentation based on deep learning still has limited success, particularly for complex structures in the abdomen. This study aimed to develop an automatic contour refinement (ACR) process to quickly correct for unacceptable auto-segmented contours.
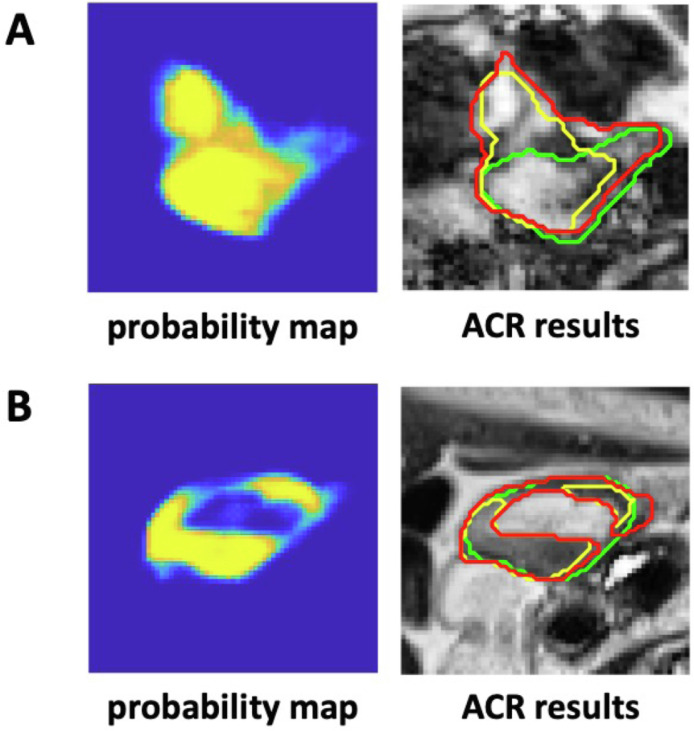
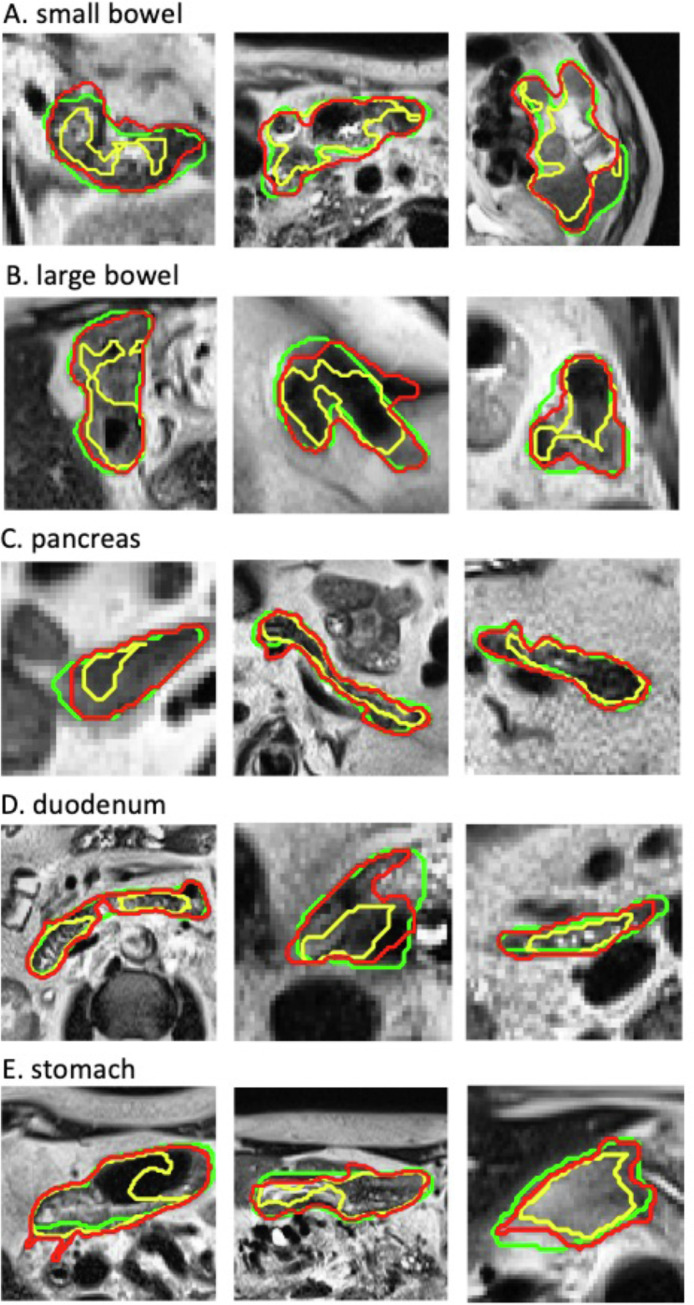
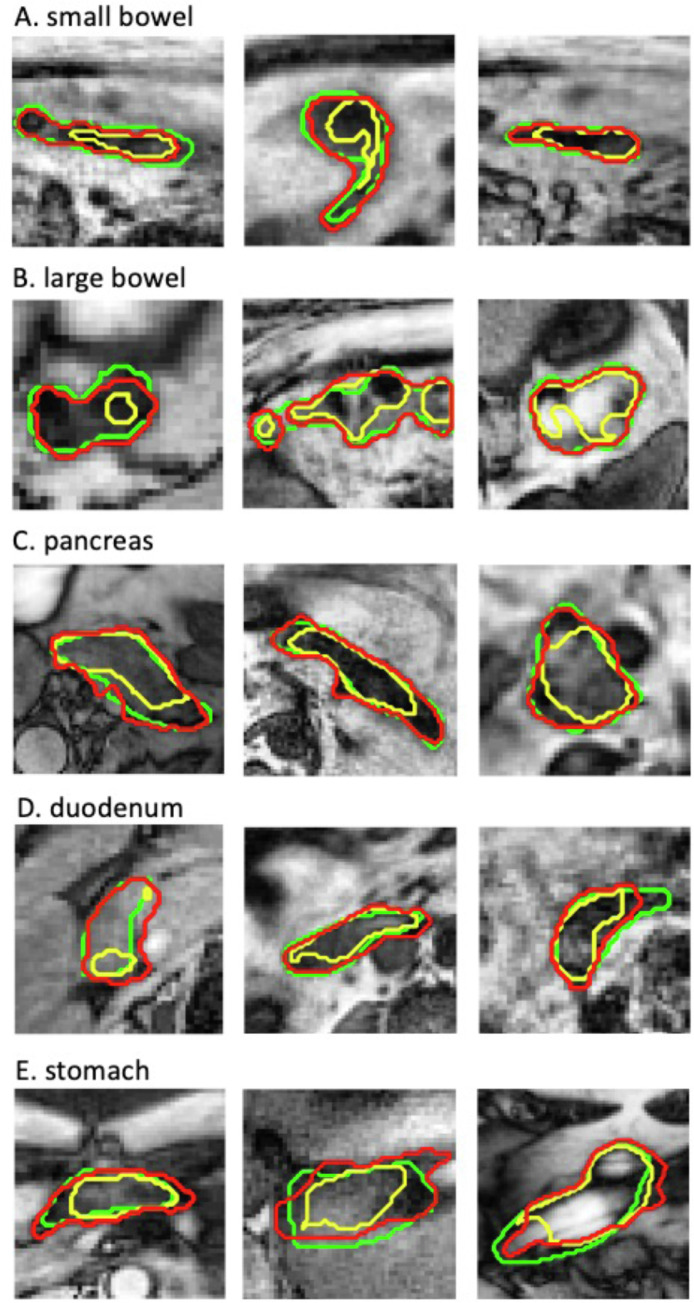
An improved level set-based active contour model (ACM) was implemented for the ACR process and was tested on the deep learning-based auto-segmentation of 80 abdominal MRI sets along with their ground truth contours. The performance of the ACR process was evaluated using 4 contour accuracy metrics: the Dice similarity coefficient (DSC), mean distance to agreement (MDA), surface DSC, and added path length (APL) on the auto-segmented contours of the small bowel, large bowel, combined bowels, pancreas, duodenum, and stomach.
A portion (3%-39%) of the corrected contours became practically acceptable per the American Association of Physicists in Medicine Task Group 132 (TG-132) recommendation (DSC >0.8 and MDA <3 mm). The best correction performance was seen in the combined bowels, where for the contours with major errors (initial DSC <0.5 or MDA >8 mm), the mean DSC increased from 0.34 to 0.59, the mean MDA decreased from 7.02 mm to 5.23 mm, and the APL reduced by almost 20 mm, whereas for the contours with minor errors, the mean DSC increased from 0.72 to 0.79, the mean MDA decreased from 3.35 mm to 3.29 mm, and more than one-third (39%) of the ACR contours became clinically acceptable. The execution time for the ACR process on one subregion was less than 2 seconds using an NVIDIA GTX 1060 GPU.
The ACR process implemented based on the ACM was able to quickly correct for some inaccurate contours produced from MRI-based deep learning auto-segmentation of complex abdominal anatomy. The ACR method may be integrated into the auto-segmentation step to accelerate the process of MRI-guided ART.
对于磁共振成像(MRI)引导的自适应放射治疗(ART)而言,对日常图像进行快速准确的自动分割至关重要。然而,基于深度学习的当前最先进的自动分割技术仍取得有限的成功,尤其是对于腹部的复杂结构。本研究旨在开发一种自动轮廓细化(ACR)流程,以快速纠正不可接受的自动分割轮廓。
为ACR流程实施了一种改进的基于水平集的主动轮廓模型(ACM),并在80套腹部MRI及其真实轮廓的基于深度学习的自动分割上进行了测试。使用4种轮廓准确性指标评估ACR流程的性能:Dice相似系数(DSC)、平均一致距离(MDA)、表面DSC和自动分割的小肠、大肠、联合肠、胰腺、十二指肠和胃轮廓上的增加路径长度(APL)。
根据医学物理师协会任务组132(TG - 132)的建议(DSC > 0.8且MDA < 3 mm),一部分(3% - 39%)校正后的轮廓实际上变得可以接受。在联合肠中观察到最佳校正性能,对于有重大误差的轮廓(初始DSC < 0.5或MDA > 8 mm),平均DSC从0.34增加到0.59,平均MDA从7.02 mm降至5.23 mm,APL减少近20 mm,而对于有轻微误差的轮廓,平均DSC从0.72增加到0.79,平均MDA从3.35 mm降至3.29 mm,超过三分之一(39%)的ACR轮廓在临床上变得可以接受。使用NVIDIA GTX 1060 GPU,ACR流程在一个子区域上的执行时间少于2秒。
基于ACM实施的ACR流程能够快速纠正基于MRI的深度学习对复杂腹部解剖结构自动分割产生的一些不准确轮廓。ACR方法可集成到自动分割步骤中,以加速MRI引导的ART进程。