Sorbonne Université, Assistance Publique-Hôpitaux de Paris (AP-HP), Hôpital La Pitié-Salpêtrière, Service de Médecine Intensive Réanimation, Paris, France.
Sorbonne Université, Assistance Publique-Hôpitaux de Paris (AP-HP), Hôpital La Pitié-Salpêtrière, Service de Médecine Intensive Réanimation, Paris, France; Sorbonne Université, Inserm, UMRS_1166-ICAN, Institut de Cardiométabolisme et Nutrition (ICAN), Paris, France; Sorbonne Université, AP-HP, Hôpital La Pitié-Salpêtrière, Institut E3M, Service de Médecine Interne 2, Centre de Référence National Lupus Systémique, Syndrome des Anticorps Anti-phospholipides et Autres Maladies Auto-Immunes Systémiques Rares, Paris, France; Sorbonne Université, Inserm, Centre d'Immunologie et des Maladies Infectieuses (CIMI-Paris), Paris, France; Sorbonne Université, AP-HP, Hôpital La Pitié-Salpêtrière, Département d'Immunologie, Paris, France.
J Am Coll Cardiol. 2022 Jul 26;80(4):299-312. doi: 10.1016/j.jacc.2022.04.056.
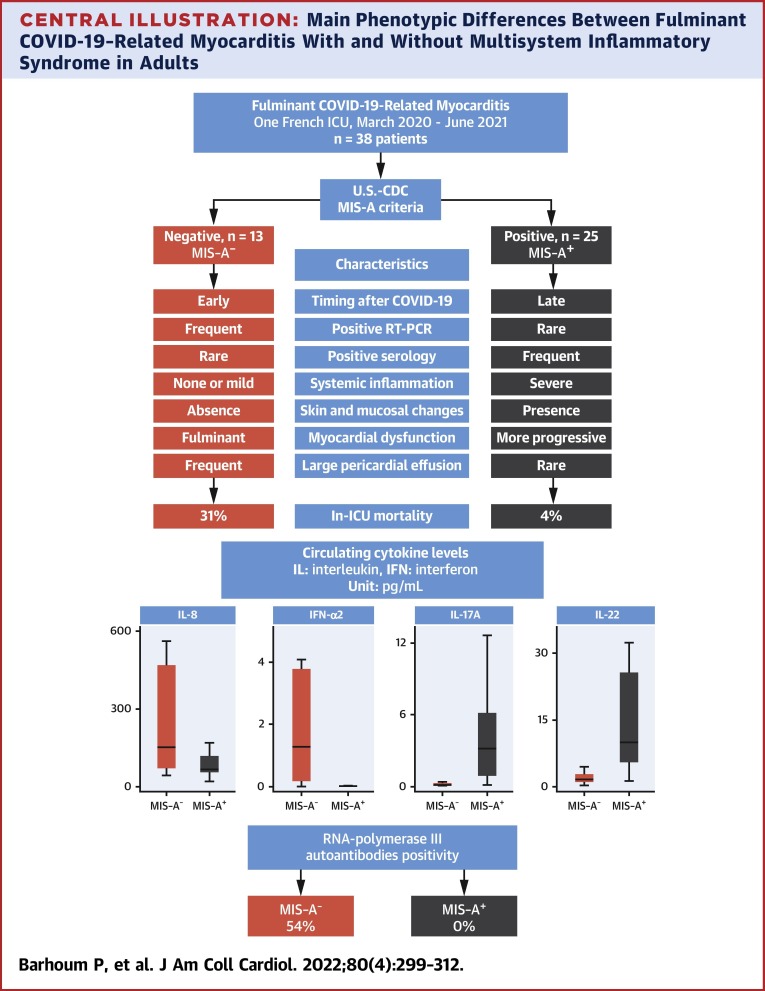
Adults who have been infected with SARS-CoV-2 can develop a multisystem inflammatory syndrome (MIS-A), including fulminant myocarditis. Yet, several patients fail to meet MIS-A criteria, suggesting the existence of distinct phenotypes in fulminant COVID-19-related myocarditis.
This study sought to compare the characteristics and clinical outcome between patients with fulminant COVID-19-related myocarditis fulfilling MIS-A criteria (MIS-A) or not (MIS-A).
A monocentric retrospective analysis of consecutive fulminant COVID-19-related myocarditis in a 26-bed intensive care unit (ICU).
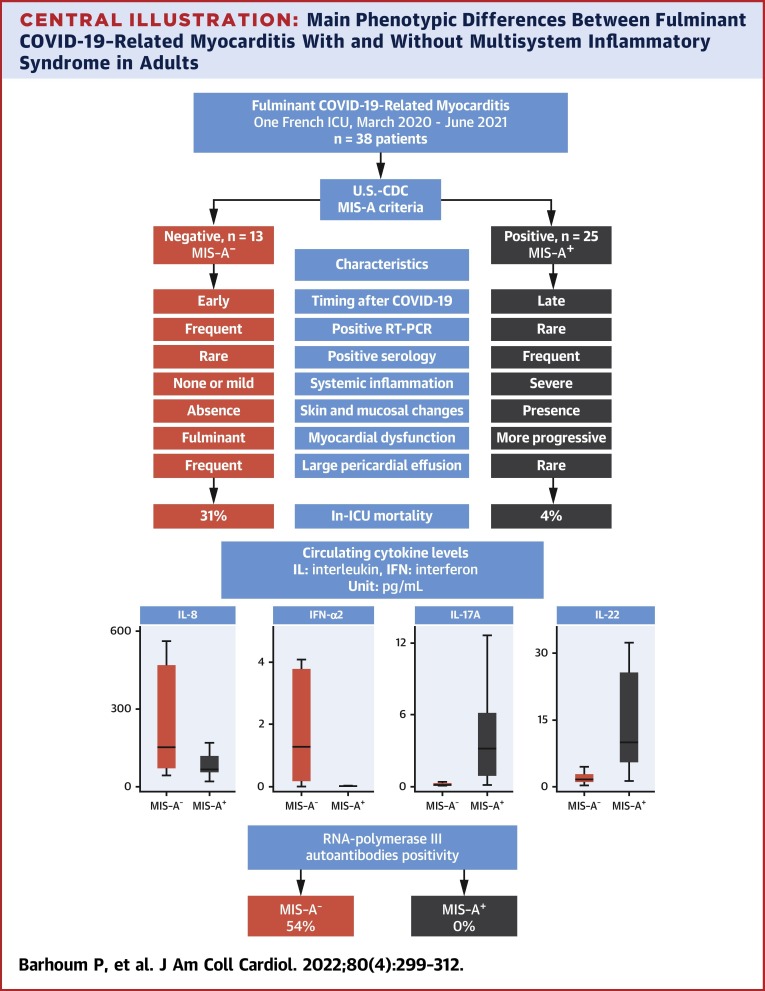
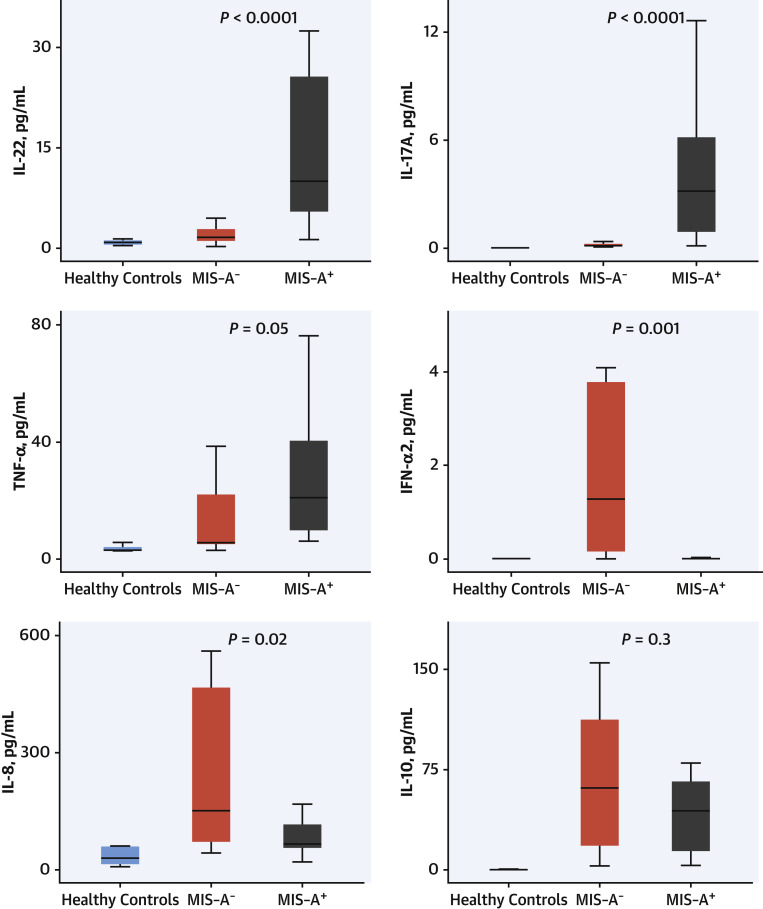
Between March 2020 and June 2021, 38 patients required ICU admission (male 66%; mean age 32 ± 15 years) for suspected fulminant COVID-19-related myocarditis. In-ICU treatment for organ failure included dobutamine 79%, norepinephrine 60%, mechanical ventilation 50%, venoarterial extracorporeal membrane oxygenation 42%, and renal replacement therapy 29%. In-hospital mortality was 13%. Twenty-five patients (66%) met the MIS-A criteria. MIS-A patients compared with MIS-A patients were characterized by a shorter delay between COVID-19 symptoms onset and myocarditis, a lower left ventricular ejection fraction, and a higher rate of in-ICU organ failure, and were more likely to require mechanical circulatory support with venoarterial extracorporeal membrane oxygenation (92% vs 16%; P < 0.0001). In-hospital mortality was higher in MIS-A patients (31% vs 4%). MIS-A had higher circulating levels of interleukin (IL)-22, IL-17, and tumor necrosis factor-α (TNF-α), whereas MIS-A had higher interferon-α2 (IFN-α2) and IL-8 levels. RNA polymerase III autoantibodies were present in 7 of 13 MIS-A patients (54%) but in none of the MIS-A patients.
MIS-A and MIS-A fulminant COVID-19-related myocarditis patients have 2 distinct phenotypes with different clinical presentations, prognosis, and immunological profiles. Differentiating these 2 phenotypes is relevant for patients' management and further understanding of their pathophysiology.
感染 SARS-CoV-2 的成年人会出现多系统炎症综合征(MIS-A),包括暴发性心肌炎。然而,一些患者不符合 MIS-A 标准,这表明暴发性 COVID-19 相关心肌炎存在不同的表型。
本研究旨在比较符合(MIS-A)或不符合(MIS-A)MIS-A 标准的暴发性 COVID-19 相关心肌炎患者的特征和临床结局。
对 26 张重症监护病房(ICU)连续收治的暴发性 COVID-19 相关心肌炎患者进行单中心回顾性分析。
2020 年 3 月至 2021 年 6 月期间,38 例患者因疑似暴发性 COVID-19 相关心肌炎需要入住 ICU(男性占 66%;平均年龄 32±15 岁)。ICU 内治疗器官衰竭包括多巴酚丁胺 79%、去甲肾上腺素 60%、机械通气 50%、静脉动脉体外膜肺氧合 42%和肾脏替代治疗 29%。院内死亡率为 13%。25 例(66%)患者符合 MIS-A 标准。与 MIS-A 患者相比,MIS-A 患者的 COVID-19 症状发作与心肌炎之间的时间间隔更短,左心室射血分数更低,ICU 内器官衰竭发生率更高,更有可能需要机械循环支持与静脉动脉体外膜肺氧合(92% vs 16%;P<0.0001)。MIS-A 患者的院内死亡率更高(31% vs 4%)。MIS-A 患者的循环白细胞介素(IL)-22、IL-17 和肿瘤坏死因子-α(TNF-α)水平较高,而 MIS-A 患者的干扰素-α2(IFN-α2)和 IL-8 水平较高。在 13 例 MIS-A 患者中有 7 例(54%)存在 RNA 聚合酶 III 自身抗体,但在 MIS-A 患者中无一例存在。
符合和不符合 MIS-A 标准的暴发性 COVID-19 相关心肌炎患者有 2 种不同的表型,临床表现、预后和免疫特征不同。区分这两种表型对患者的管理和进一步了解其病理生理学具有重要意义。