Well Living House (Smylie, McConkey, Brar), St. Michael's Hospital; Dalla Lana School of Public Health (Smylie, McConkey, Rachlis, Avery), University of Toronto; ICES (Smylie, Rachlis, Mecredy); Princess Margaret Cancer Centre (Avery), University Health Network; Seventh Generations Midwives Toronto (Bourgeois); Call Auntie Clinic (Bourgeois); School of Kinesiology and Health Science (Rotondi), York University, Toronto, Ont.; Southwest Ontario Aboriginal Health Access Centre (Dokis, Vandevenne), London, Ont.
CMAJ. 2022 Aug 2;194(29):E1018-E1026. doi: 10.1503/cmaj.212147.
First Nations, Inuit and Métis Peoples across geographies are at higher risk of SARS-CoV-2 infection and COVID-19 because of high rates of chronic disease, inadequate housing and barriers to accessing health services. Most Indigenous Peoples in Canada live in cities, where SARS-CoV-2 infection is concentrated. To address gaps in SARS-CoV-2 information for these urban populations, we partnered with Indigenous agencies and sought to generate rates of SARS-CoV-2 testing and vaccination, and incidence of infection for First Nations, Inuit and Métis living in 2 Ontario cities.
We drew on existing cohorts of First Nations, Inuit and Métis adults in Toronto ( = 723) and London ( = 364), Ontario, who were recruited using respondent-driven sampling. We linked to ICES SARS-CoV-2 databases and prospectively monitored rates of SARS-CoV-2 testing, diagnosis and vaccination for First Nations, Inuit and Métis, and comparator city and Ontario populations.
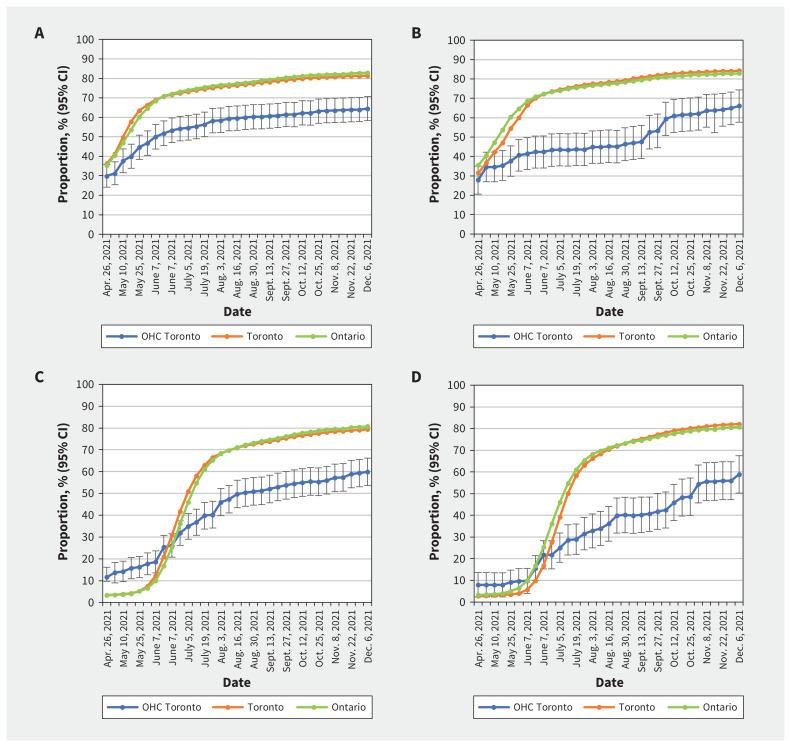
We found that SARS-CoV-2 testing rates among First Nations, Inuit and Métis were higher in Toronto (54.7%, 95% confidence interval [CI] 48.1% to 61.3%) and similar in London (44.5%, 95% CI 36.0% to 53.1%) compared with local and provincial rates. We determined that cumulative incidence of SARS-CoV-2 infection was not significantly different among First Nations, Inuit and Métis in Toronto (7364/100 000, 95% CI 2882 to 11 847) or London (7707/100 000, 95% CI 2215 to 13 200) compared with city rates. We found that rates of vaccination among First Nations, Inuit and Métis in Toronto (58.2%, 95% CI 51.4% to 64.9%) and London (61.5%, 95% CI 52.9% to 70.0%) were lower than the rates for the 2 cities and Ontario.
Although Ontario government policies prioritized Indigenous populations for SARS-CoV-2 vaccination, vaccine uptake was lower than in the general population for First Nations, Inuit and Métis Peoples in Toronto and London. Ongoing access to culturally safe testing and vaccinations is urgently required to avoid disproportionate hospital admisson and mortality related to COVID-19 in these communities.
由于慢性病发病率高、住房条件不足以及获得医疗服务的障碍,各地的第一民族、因纽特人和梅蒂斯人感染 SARS-CoV-2 和 COVID-19 的风险更高。加拿大的大多数土著人居住在城市,那里是 SARS-CoV-2 感染的集中地。为了解决这些城市人口中 SARS-CoV-2 信息方面的差距,我们与土著机构合作,试图为在安大略省两个城市居住的第一民族、因纽特人和梅蒂斯人确定 SARS-CoV-2 检测和疫苗接种率以及感染发病率。
我们利用多伦多(=723)和伦敦(=364)的现有第一民族、因纽特人和梅蒂斯成年人队列,这些人是通过回应驱动抽样招募的。我们与安大略省癌症研究所的 SARS-CoV-2 数据库相关联,并对第一民族、因纽特人和梅蒂斯人的 SARS-CoV-2 检测、诊断和疫苗接种率以及比较城市和安大略省人群进行了前瞻性监测。
我们发现,多伦多的第一民族、因纽特人和梅蒂斯人的 SARS-CoV-2 检测率较高(54.7%,95%置信区间[CI]48.1%至 61.3%),而伦敦的 SARS-CoV-2 检测率相似(44.5%,95%CI36.0%至 53.1%),与当地和省级水平相比。我们确定,在多伦多(7364/100000,95%CI2882 至 11847)或伦敦(7707/100000,95%CI2215 至 13200),第一民族、因纽特人和梅蒂斯人的 SARS-CoV-2 累计感染发病率与城市水平相比没有显著差异。我们发现,多伦多(58.2%,95%CI51.4%至 64.9%)和伦敦(61.5%,95%CI52.9%至 70.0%)第一民族、因纽特人和梅蒂斯人的疫苗接种率低于这两个城市和安大略省的水平。
尽管安大略省政府的政策优先考虑了第一民族人群的 SARS-CoV-2 疫苗接种,但在多伦多和伦敦,第一民族、因纽特人和梅蒂斯人的疫苗接种率低于一般人群。为避免这些社区因 COVID-19 而出现不成比例的住院和死亡,迫切需要持续获得文化安全的检测和疫苗接种。