Department of Health Services, Policy, and Practice, Brown University School of Public Health, Providence, Rhode Island.
Providence VA Medical Center, Providence, Rhode Island.
JAMA Health Forum. 2021 Jun 11;2(6):e210793. doi: 10.1001/jamahealthforum.2021.0793. eCollection 2021 Jun.
Medicare Advantage (MA) plans, which disproportionately enroll racial/ethnic minorities and persons with socioeconomic disadvantage, receive bonus payments on the basis of overall performance on a 5-star rating scale. The association between plans' overall quality and disparities in quality is not well understood.
To examine the association between MA star ratings and disparities in care for racial/ethnic minorities and enrollees with lower income and educational attainment.
This cross-sectional study included 1 578 564 MA enrollees from 454 contracts across the 2015 and 2016 calendar years. Data analyses were conducted between June 2019 and June 2020.
Self-reported race and ethnicity and low socioeconomic status (SES) (defined by low income or less than a high school education) vs high SES (neither low income nor low educational attainment).
Performance on 22 measures of quality and satisfaction determined at the individual enrollee level, aggregated into simulated star ratings (scale, 2-5) stratified by SES and race/ethnicity.
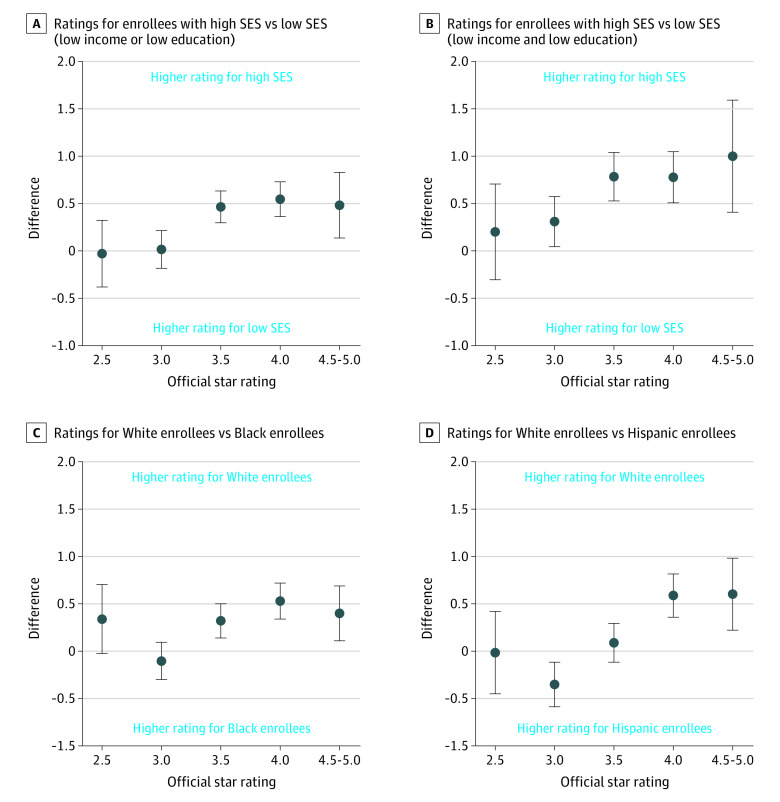
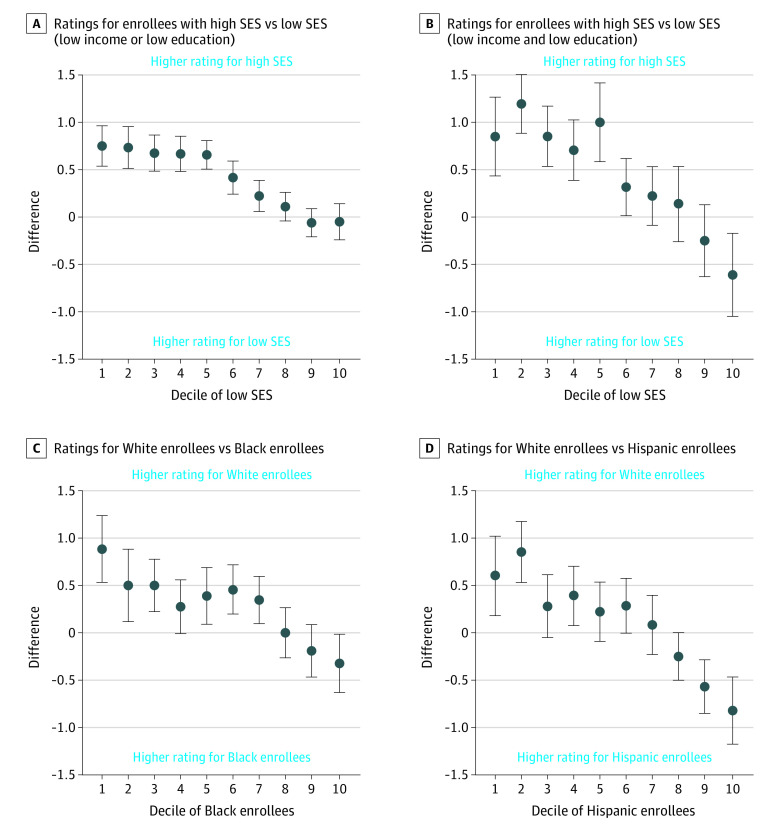
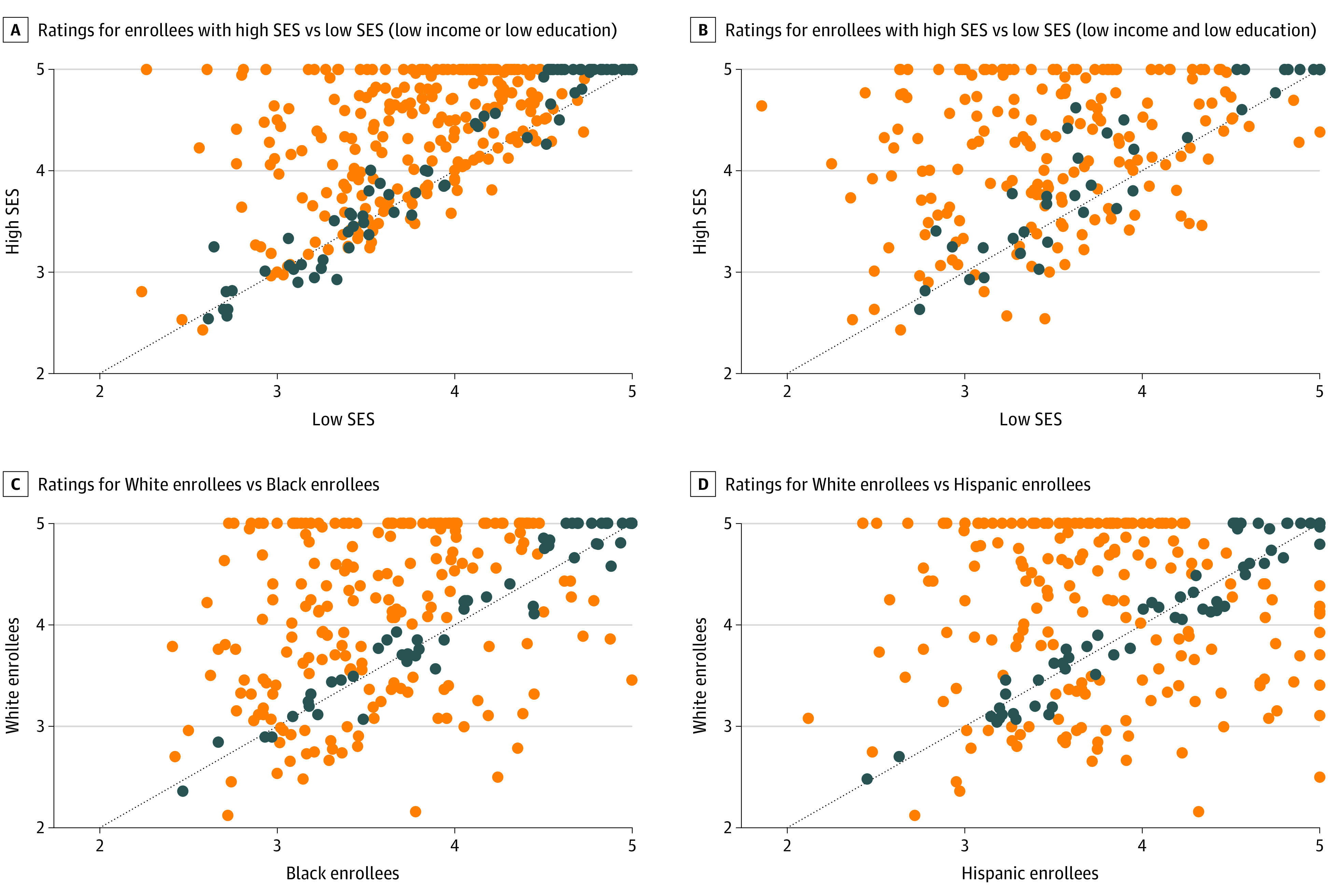
A total of 1 578 564 enrollees were included in this analysis (55.8% female; mean [SD] age, 71.4 [11.3] years; 65.8% White; 12.3% Black; 14.6% Hispanic). Enrollees with low SES had simulated stratified star ratings 0.5 stars lower (95% CI, 0.4-0.6 stars) than individuals with high SES in the same contract. Black and Hispanic enrollees had simulated star ratings that were 0.3 stars (95% CI, 0.2-0.4 stars) and 0.1 stars (95% CI, -0.04 to 0.2 stars) lower than White enrollees within the same contracts. Black enrollees had a 0.4-star lower rating (95% CI, 0.1-0.7 stars) in 4.5- to 5-star contracts and a no statistical difference in 2.0- to 2.5-star-rated contracts (difference, 0.3 stars; 95% CI, -0.02 to 0.7 stars). Hispanic enrollees had a 0.6-star lower simulated rating (95% CI, 0.2-1.0 stars) in 4.5- to 5-star contracts and no statistical difference in 2- to 2.5-star contracts (difference, -0.01 stars; 95% CI, -0.5 to 0.4 stars). There was low correlation between simulated ratings for enrollees of low SES and high SES (difference, 0.2 stars; 95% CI, 0.03-0.4 stars) and between simulated ratings for White and Black enrollees (difference, 0.4 stars; 95% CI, 0.3-0.5 stars) and White and Hispanic enrollees (difference, 0.3 stars; 95% CI, 0.2-0.4 stars). As the proportion of Black and Hispanic enrollees increased in a contract, racial/ethnic disparities in ratings decreased.
In this cross-sectional study, simulated MA star ratings were only weakly correlated with those for enrollees of low SES in the same contract, and contracts with higher star ratings had larger disparities in quality. Measures of equity in MA plans' quality of care may be needed.
重要性:医疗保险优势(MA)计划在总体绩效五星评级制度基础上获得额外奖金,这些计划中包含了不成比例的少数民族和社会经济处于劣势的人群。人们对计划整体质量与护理质量差异之间的关联了解甚少。
目的:研究 MA 星级评定与少数民族和收入较低、教育程度较低的参保者之间的护理质量差异之间的关系。
设计、地点和参与者:本横断面研究纳入了来自 2015 年和 2016 年日历年度的 454 份合同中的 1578564 名 MA 参保者。数据分析于 2019 年 6 月至 2020 年 6 月进行。
暴露因素:自我报告的种族和民族以及低社会经济地位(SES)(定义为低收入或未完成高中学业)与高 SES(既不是低收入也不是低教育程度)相对。
主要结果和措施:对 22 项个体参保者层面的质量和满意度指标进行了评估,这些指标按 SES 和种族/民族进行了分层,汇总为模拟星级评定(评分范围为 2-5 星)。
结果:本分析共纳入 1578564 名参保者(55.8%为女性;平均[标准差]年龄为 71.4[11.3]岁;65.8%为白人;12.3%为黑人;14.6%为西班牙裔)。在同一合同中,SES 较低的参保者的模拟分层星级评定低 0.5 星(95%置信区间,0.4-0.6 星)。在同一合同中,与白人参保者相比,黑人参保者和西班牙裔参保者的模拟星级评定低 0.3 星(95%置信区间,0.2-0.4 星)和 0.1 星(95%置信区间,-0.04 至 0.2 星)。黑人参保者在 4.5 星至 5 星合同中的评级低 0.4 星(95%置信区间,0.1-0.7 星),而在 2.0 星至 2.5 星评级合同中没有统计学差异(差异为 0.3 星;95%置信区间,-0.02 至 0.7 星)。西班牙裔参保者在 4.5 星至 5 星合同中的模拟评分低 0.6 星(95%置信区间,0.2-1.0 星),在 2.0 星至 2.5 星合同中没有统计学差异(差异为-0.01 星;95%置信区间,-0.5 至 0.4 星)。SES 较低的参保者和 SES 较高的参保者的模拟评分之间的相关性较低(差异为 0.2 星;95%置信区间,0.03-0.4 星),以及白人参保者和黑人参保者(差异为 0.4 星;95%置信区间,0.3-0.5 星)和白人参保者和西班牙裔参保者(差异为 0.3 星;95%置信区间,0.2-0.4 星)的模拟评分之间的相关性较低。随着合同中黑人参保者和西班牙裔参保者比例的增加,评分中的种族/民族差异也随之减少。
结论和相关性:在这项横断面研究中,模拟的 MA 星级评定与同一合同中 SES 较低的参保者的评分仅存在微弱相关性,而星级评定较高的合同的质量差异更大。医疗保险优势计划护理质量公平措施可能是必要的。