Menzies School of Health Research, Darwin, NT, Australia.
Centre for Epidemiology and Biostatistics, Melbourne School of Population and Global Health, University of Melbourne, Melbourne, VIC, Australia.
Clin Drug Investig. 2023 Jan;43(1):23-33. doi: 10.1007/s40261-022-01204-z. Epub 2022 Oct 10.
Clinical risk factors for nephrotoxicity in Staphylococcus aureus bacteraemia remain largely undetermined, despite its common occurrence and clinical significance. In an international, multicentre, prospective clinical trial (CAMERA2), which compared standard therapy (vancomycin monotherapy) to combination therapy (adding an anti-staphylococcal beta-lactam) for methicillin-resistant S. aureus bacteraemia, significantly more people in the combination therapy arm experienced acute kidney injury compared with those in the monotherapy arm (23% vs 6%).
The aim of this post hoc analysis was to explore in greater depth the risk factors for acute kidney injury from the CAMERA2 trial.
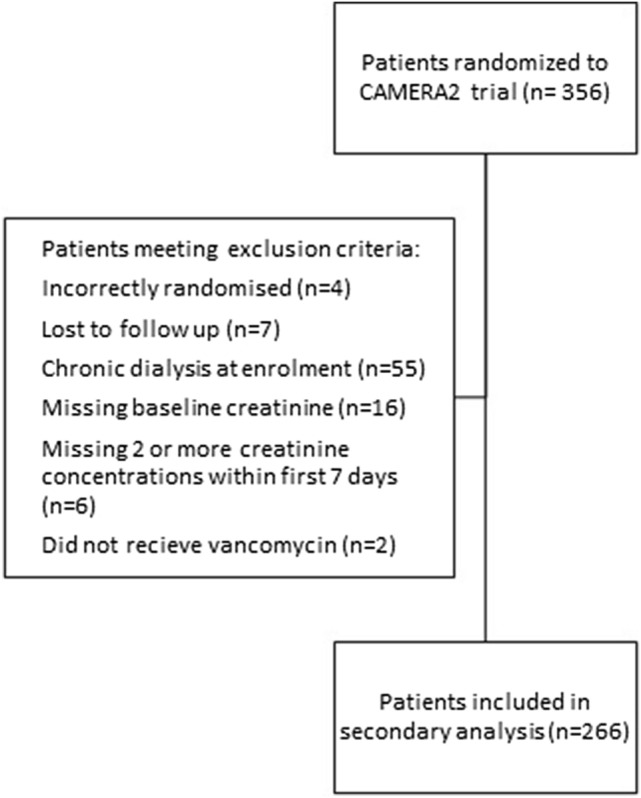
Among participants of the CAMERA2 trial, demographic-related, infection-related and treatment-related risk factors were assessed for their relationship with acute kidney injury by univariable and multivariable logistic regression. Acute kidney injury was defined by a modified-KDIGO (Kidney Disease: Improving Global Outcomes) criteria (not including urinary output).
Of the 266 participants included, age (p = 0.04), randomisation to combination therapy (p = 0.002), vancomycin area under the concentration-time curve (p = 0.03) and receipt of (flu)cloxacillin as the companion beta-lactam (p < 0.001) were significantly associated with acute kidney injury. On a multivariable analysis, concurrent use of (flu)cloxacillin increased the risk of acute kidney injury over four times compared with the use of cefazolin or no beta-lactam. The association of vancomycin area under the concentration-time curve with acute kidney injury also persisted in the multivariable model.
For participants receiving vancomycin for S. aureus bacteraemia, use of (flu)cloxacillin and increased vancomycin area under the concentration-time curve were risk factors for acute kidney injury. These represent potentially modifiable risk factors for nephrotoxicity and highlight the importance of avoiding the use of concurrent nephrotoxins.
金黄色葡萄球菌菌血症的肾毒性的临床危险因素在很大程度上仍未确定,尽管其发生较为常见,且具有重要的临床意义。在一项比较耐甲氧西林金黄色葡萄球菌菌血症的标准治疗(万古霉素单药治疗)与联合治疗(添加抗葡萄球菌β-内酰胺类药物)的国际多中心前瞻性临床试验(CAMERA2)中,联合治疗组发生急性肾损伤的人数明显多于单药治疗组(23% vs 6%)。
本事后分析旨在更深入地探讨 CAMERA2 试验中导致急性肾损伤的危险因素。
在 CAMERA2 试验的参与者中,通过单变量和多变量逻辑回归评估与急性肾损伤相关的人口统计学相关、感染相关和治疗相关的危险因素。根据改良的 KDIGO(肾脏疾病:改善全球预后)标准(不包括尿量)定义急性肾损伤。
在 266 名参与者中,年龄(p = 0.04)、随机分配至联合治疗组(p = 0.002)、万古霉素浓度-时间曲线下面积(p = 0.03)和接受(氟)氯唑西林作为联合β-内酰胺类药物(p < 0.001)与急性肾损伤显著相关。在多变量分析中,与使用头孢唑林或无β-内酰胺类药物相比,同时使用(氟)氯唑西林使急性肾损伤的风险增加了四倍以上。万古霉素浓度-时间曲线下面积与急性肾损伤的相关性在多变量模型中仍然存在。
对于接受万古霉素治疗的金黄色葡萄球菌菌血症患者,使用(氟)氯唑西林和增加万古霉素浓度-时间曲线下面积是急性肾损伤的危险因素。这些因素代表潜在可改变的肾毒性危险因素,并强调了避免同时使用肾毒性药物的重要性。