Sherif Noha, Khine Kay T, Houghton Odette M
University of North Carolina School of Medicine, Chapel Hill, NC, USA.
Bascom Palmer Eye Institute, University of Miami School of Medicine, Miami, FL, USA.
Am J Ophthalmol Case Rep. 2022 Sep 13;28:101695. doi: 10.1016/j.ajoc.2022.101695. eCollection 2022 Dec.
To report the case of an immunocompetent 62-year old woman with acute syphilitic posterior placoid chorioretinitis.
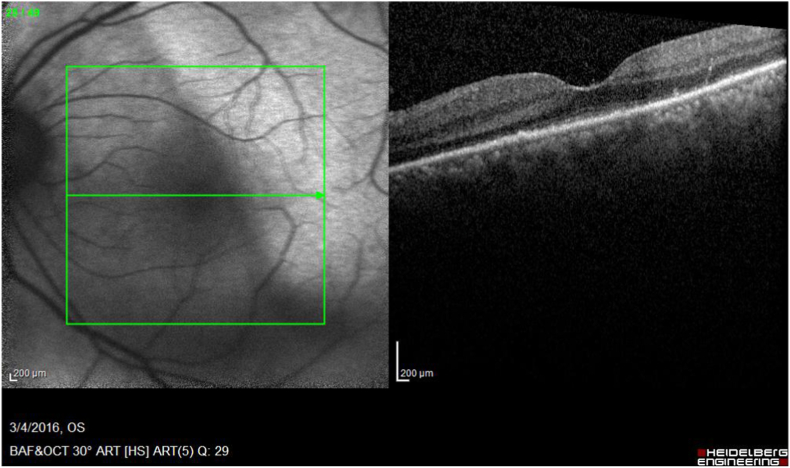
The patient presented with sudden, painless vision loss in the left eye (OS) four months after self-resolving decreased vision in the right eye (OD) which was incorrectly attributed to ischemic optic neuropathy. At the time of presentation, visual acuity (VA) was hand motion OS and 20/30 OD. The dilated fundus exam demonstrated a flat, yellow-white macular lesion, deep to the retinal vasculature with a temporal, curvilinear demarcation line OS and was unremarkable OD. Trace vitreous cells and veils OS were observed. Optical coherence tomography demonstrated loss of photoreceptor layers. Rapid plasma reagin and fluorescent treponemal antibody absorption were positive. The patient was treated with intravenous penicillin and prednisolone acetate drops with resolution of vitreous cells and return of VA.
Acute syphilitic posterior placoid chorioretinitis can be the single presenting symptom in syphilis. It is imperative for ophthalmologists to consider this relatively uncommon manifestation of syphilis in the differential in immunocompetent patients presenting with unsuspecting histories and perplexing vision loss.
报告一例免疫功能正常的62岁女性急性梅毒性后极部扁平状脉络膜视网膜炎病例。
患者右眼视力下降自行缓解4个月后,左眼突然无痛性视力丧失,右眼视力下降最初被误诊为缺血性视神经病变。就诊时,左眼视力为手动,右眼视力为20/30。散瞳眼底检查发现左眼有一个扁平的黄白色黄斑病变,位于视网膜血管深层,颞侧有一条曲线状分界线,右眼未见明显异常。左眼可见少量玻璃体细胞和混浊物。光学相干断层扫描显示光感受器层缺失。快速血浆反应素试验和荧光密螺旋体抗体吸收试验均为阳性。患者接受静脉注射青霉素和醋酸泼尼松龙滴眼液治疗,玻璃体细胞消失,视力恢复。
急性梅毒性后极部扁平状脉络膜视网膜炎可能是梅毒的唯一表现症状。对于有不明病史和令人困惑的视力丧失的免疫功能正常患者,眼科医生在鉴别诊断时必须考虑梅毒这种相对罕见的表现。