MRC Unit for Lifelong Health and Ageing, UCL, London, UK
Centre for Longitudinal Studies, Social Research Institute, UCL, London, UK.
BMJ Open. 2022 Oct 13;12(10):e064981. doi: 10.1136/bmjopen-2022-064981.
We investigated associations between multiple sociodemographic characteristics (sex, age, occupational social class, education and ethnicity) and self-reported healthcare disruptions during the early stages of the COVID-19 pandemic.
Coordinated analysis of prospective population surveys.
Community-dwelling participants in the UK between April 2020 and January 2021.
Over 68 000 participants from 12 longitudinal studies.
Self-reported healthcare disruption to medication access, procedures and appointments.
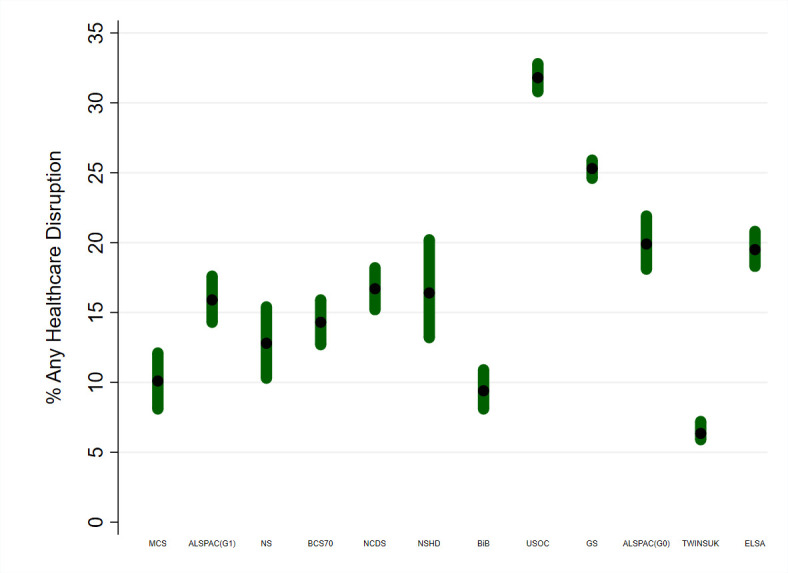
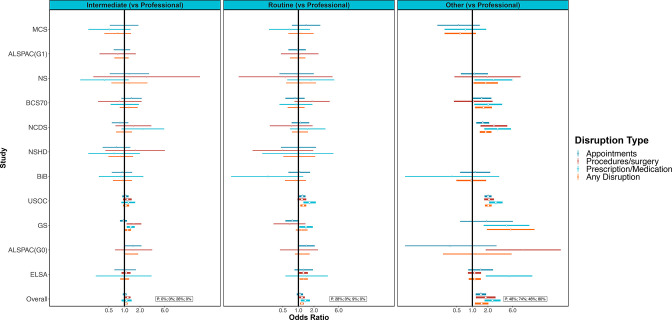
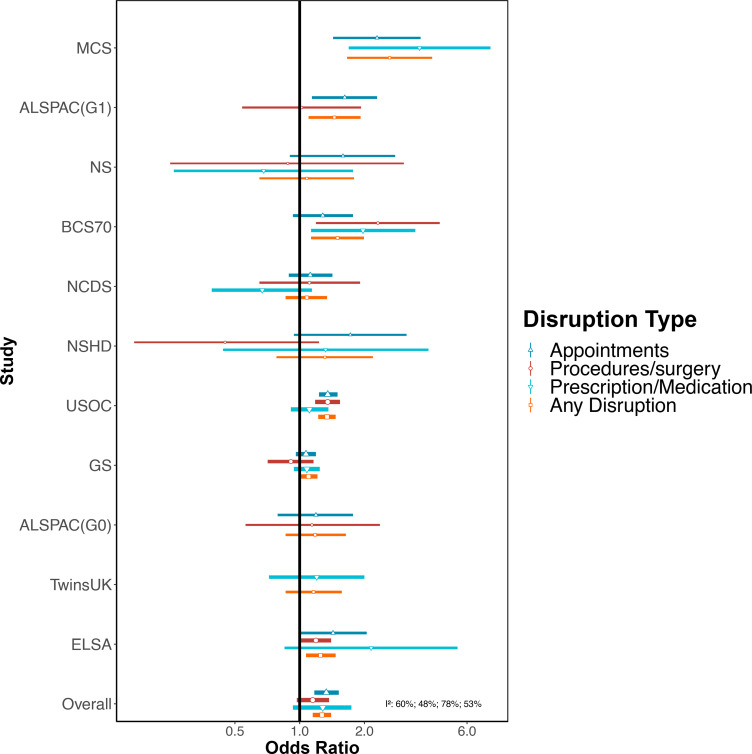
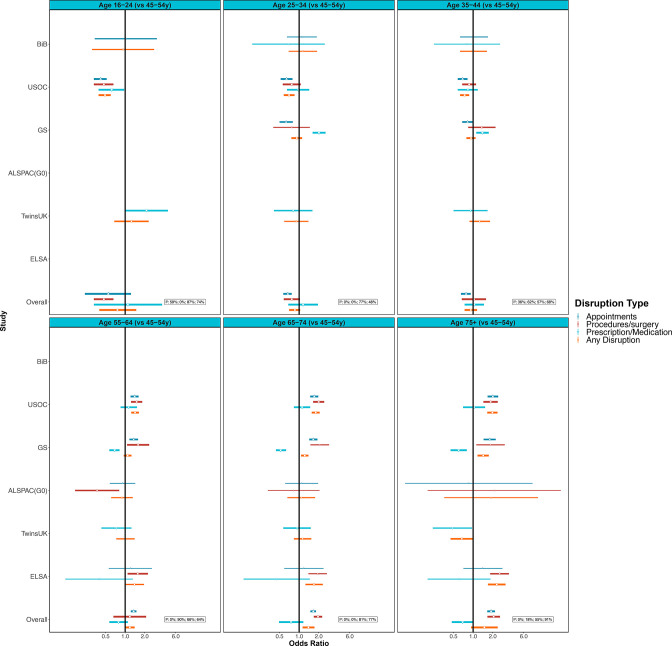
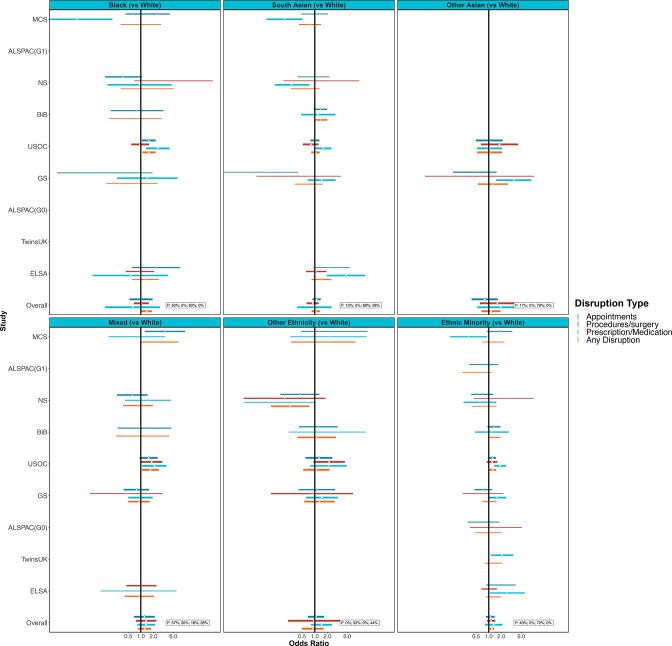
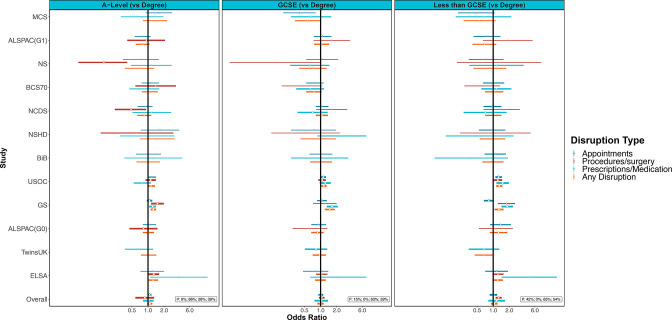
Prevalence of healthcare disruption varied substantially across studies: between 6% and 32% reported any disruption, with 1%-10% experiencing disruptions in medication, 1%-17% experiencing disruption in procedures and 4%-28% experiencing disruption in clinical appointments. Females (OR 1.27; 95% CI 1.15 to 1.40; I=54%), older persons (eg, OR 1.39; 95% CI 1.13 to 1.72; I=77% for 65-75 years vs 45-54 years) and ethnic minorities (excluding white minorities) (OR 1.19; 95% CI 1.05 to 1.35; I=0% vs white) were more likely to report healthcare disruptions. Those in a more disadvantaged social class were also more likely to report healthcare disruptions (eg, OR 1.17; 95% CI 1.08 to 1.27; I=0% for manual/routine vs managerial/professional), but no clear differences were observed by education. We did not find evidence that these associations differed by shielding status.
Healthcare disruptions during the COVID-19 pandemic could contribute to the maintenance or widening of existing health inequalities.
我们调查了多种社会人口学特征(性别、年龄、职业社会阶层、教育程度和种族)与 COVID-19 大流行早期报告的医疗保健中断之间的关联。
对前瞻性人群调查进行协调分析。
2020 年 4 月至 2021 年 1 月期间居住在英国的社区居民。
来自 12 项纵向研究的超过 68000 名参与者。
报告的医疗保健中断包括药物获取、程序和预约。
研究之间的医疗保健中断发生率差异很大:报告任何中断的比例为 6%-32%,1%-10%的人药物中断,1%-17%的人程序中断,4%-28%的人临床预约中断。女性(比值比 1.27;95%置信区间 1.15 至 1.40;I=54%)、老年人(例如,比值比 1.39;95%置信区间 1.13 至 1.72;I=77%,65-75 岁与 45-54 岁相比)和少数民族(不包括白人少数民族)(比值比 1.19;95%置信区间 1.05 至 1.35;I=0%与白人相比)更有可能报告医疗保健中断。处于社会地位较低的阶层的人也更有可能报告医疗保健中断(例如,比值比 1.17;95%置信区间 1.08 至 1.27;I=0%,体力/常规与管理/专业相比),但教育程度没有明显差异。我们没有发现这些关联因屏蔽状态而异的证据。
COVID-19 大流行期间的医疗保健中断可能导致现有的健康不平等状况得以维持或扩大。