Liu Xue, Xiao Zhenghua, Cheng Lan, Jian Luhong
Department of Obstetrics, Yongchuan Hospital of Chongqing Medical University, Chongqing 402160, China.
J Clin Transl Res. 2022 Nov 10;8(6):516-522. eCollection 2022 Dec 29.
This study aims to investigate thyroid function-associated parameters and the incidence of thyroid disorders in pregnant women, with the overarching aim to ensure that pregnant women do not develop said disorders due to aberrant iodine levels during the course of pregnancy.
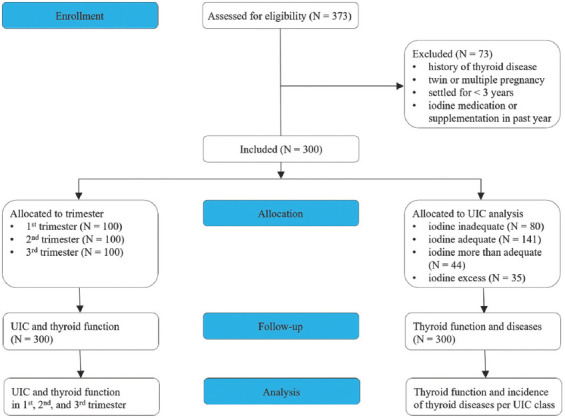
A total of 300 pregnant women who underwent routine check-ups at the Yongchuan Hospital Affiliated to Chongqing Medical University from January to December 2021 were enrolled. Venous blood and morning urine were collected. Serum thyroid-stimulating hormone (TSH), free thyroxine (FT4), and free triiodothyronine (FT3) were determined by chemiluminescence immunoassay. Urinary iodine concentration (UIC) was detected by arsenic cerium catalytic spectrophotometry. Thyroid disorders were extrapolated from the measured parameters.
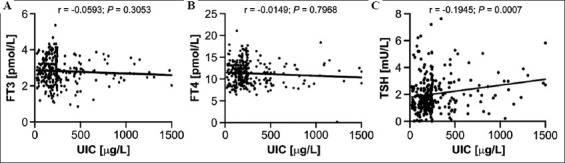
The overall median UIC was 203 μg/L, which was within normal range. Subgroup analysis revealed that the median UIC in the first trimester was 187.5 μg/L, 211.8 μg/L in the second trimester, and 239.9 μg/L in the third trimester. However, based on the WHO criteria, 32%, 30%, and 18% of pregnant women were iodine deficient during their first, second, and third trimester, respectively. The proportion of women with iodine deficiency in the first and second trimesters was higher compared to the third trimester (P < 0.05). Serum FT3 and FT4 concentrations were higher in subjects in their first and second trimester versus the third trimester, while serum TSH levels were lower in subjects in their first and second trimester versus the third trimester (P < 0.05). The TSH concentration in subjects with inadequate iodine intake (UIC < 150 μg/L) was lower compared to subjects with adequate iodine intake (UIC 150 - 249 μg/L), but higher than in subjects with more than adequate intake (UIC 250 - 499 μg/L) and excess iodine intake (UIC ≥ 500 μg/L) (P < 0.05). TSH concentration and UIC were positively correlated (r = 0.1945, P = 0.0007), while no relationship was observed between UIC and FT3 and FT4 serum levels (r = -0.0593, P = 0.3053; r = -0.0149, P = 0.7968). There was no significant difference in FT3 and FT4 concentration between different UIC strata (P > 0.05). The incidence of thyroid disease during pregnancy in iodine-deficient women was greater compared to pregnant women with adequate iodine intake (P < 0.05) and higher in subjects in the more than adequate as well as excessive iodine intake cohorts (P < 0.05).
The iodine nutritional intake by pregnant women in Yongchuan District, Chongqing, was generally sufficient to meet developmental and metabolic needs. However, about a third of women in their first and second trimester exhibited iodine deficiency. Iodine deficiency was associated with an increased incidence of thyroid diseases.
In clinical practice, the UIC of pregnant women should be measured during key stages in the pregnancy to prevent the manifestation of thyroid diseases.
本研究旨在调查孕妇甲状腺功能相关参数及甲状腺疾病的发病率,总体目标是确保孕妇在孕期不会因碘水平异常而患上上述疾病。
选取2021年1月至12月在重庆医科大学附属永川医院进行常规检查的300名孕妇。采集静脉血和晨尿。采用化学发光免疫分析法测定血清促甲状腺激素(TSH)、游离甲状腺素(FT4)和游离三碘甲状腺原氨酸(FT3)。采用砷铈催化分光光度法检测尿碘浓度(UIC)。根据测量参数推断甲状腺疾病情况。
总体UIC中位数为203μg/L,处于正常范围内。亚组分析显示,孕早期UIC中位数为187.5μg/L,孕中期为211.8μg/L,孕晚期为239.9μg/L。然而,根据世界卫生组织标准,分别有32%、30%和18%的孕妇在孕早期、孕中期和孕晚期碘缺乏。孕早期和孕中期碘缺乏女性的比例高于孕晚期(P<0.05)。孕早期和孕中期受试者的血清FT3和FT4浓度高于孕晚期,而孕早期和孕中期受试者的血清TSH水平低于孕晚期(P<0.05)。碘摄入不足(UIC<μg/L)受试者的TSH浓度低于碘摄入充足(UIC 150 - 249μg/L)的受试者,但高于碘摄入过量(UIC 250 - 499μg/L)和碘摄入过多(UIC≥500μg/L)的受试者(P<0.05)。TSH浓度与UIC呈正相关(r = 0.1945,P = 0.0007),而未观察到UIC与血清FT3和FT4水平之间存在关联(r = -0.0593,P = 0.3053;r = -0.0149,P = 0.7968)。不同UIC分层之间FT3和FT4浓度无显著差异(P>0.05)。碘缺乏女性孕期甲状腺疾病的发病率高于碘摄入充足的孕妇(P<0.05),在碘摄入过量及碘摄入过多的人群中发病率也更高(P<0.05)。
重庆永川区孕妇的碘营养摄入量总体上足以满足发育和代谢需求。然而,约三分之一的孕早期和孕中期女性存在碘缺乏。碘缺乏与甲状腺疾病发病率增加有关。
在临床实践中,应在孕期关键阶段测量孕妇的UIC,以预防甲状腺疾病的发生。