Arvola Samuli, Seppänen Marko, Timonen Kirsi L, Rautio Pentti, Ettala Otto, Anttinen Mikael, Boström Peter J, Noponen Tommi
Department of Clinical Physiology, Nuclear Medicine and Turku PET Centre, Turku University Hospital and University of Turku, Kiinamyllynkatu 4-8, P.O. Box 52, 20521, Turku, Finland.
Department of Clinical Physiology and Nuclear Medicine, Hospital Nova of Central Finland, Jyväskylä, Finland.
EJNMMI Phys. 2022 Dec 12;9(1):85. doi: 10.1186/s40658-022-00517-4.
We evaluated the effects of acquisition time, energy window width, and matrix size on the image quality, quantitation, and diagnostic performance of whole-body Tc-HMDP SPECT/CT in the primary metastasis staging of prostate cancer.
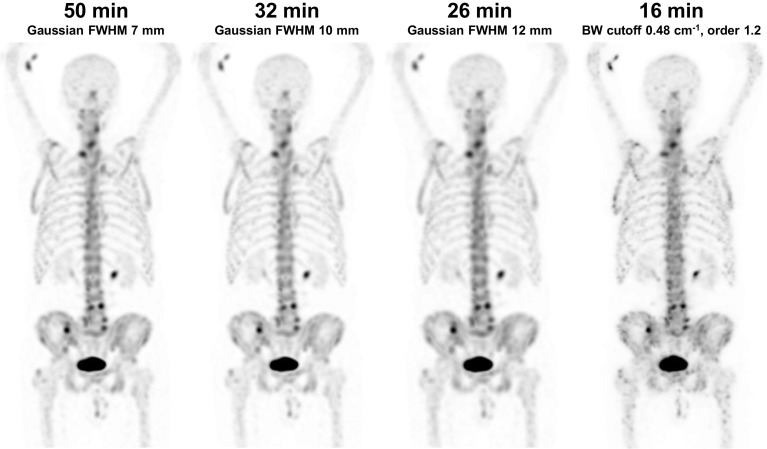
Thirty prostate cancer patients underwent Tc-HMDP SPECT/CT from the top of the head to the mid-thigh using a Discovery NM/CT 670 CZT system with list-mode acquisition, 50-min acquisition time, 15% energy window width, and 128 × 128 matrix size. The acquired list-mode data were resampled to produce data sets with shorter acquisition times of 41, 38, 32, 26, 20, and 16 min, narrower energy windows of 10, 8, 6, and 4%, and a larger matrix size of 256 × 256. Images were qualitatively evaluated by three experienced nuclear medicine physicians and quantitatively evaluated by noise, lesion contrast and SUV measurements. Diagnostic performance was evaluated from the readings of two experienced nuclear medicine physicians in terms of patient-, region-, and lesion-level sensitivity and specificity.
The originally acquired images had the best qualitative image quality and lowest noise. However, the acquisition time could be reduced to 38 min, the energy window narrowed to 8%, and the matrix size increased to 256 × 256 with still acceptable qualitative image quality. Lesion contrast and SUVs were not affected by changes in acquisition parameters. Acquisition time reduction had no effect on the diagnostic performance, as sensitivity, specificity, accuracy, and area under the receiver-operating characteristic curve were not significantly different between the 50-min and reduced acquisition time images. The average patient-level sensitivities of the two readers were 88, 92, 100, and 96% for the 50-, 32-, 26-, and 16-min images, respectively, and the corresponding specificities were 78, 84, 84, and 78%. The average region-level sensitivities of the two readers were 55, 58, 59, and 56% for the 50-, 32-, 26-, and 16-min images, respectively, and the corresponding specificities were 95, 98, 96, and 95%. The number of equivocal lesions tended to increase as the acquisition time decreased.
Whole-body Tc-HMDP SPECT/CT can be acquired using a general-purpose CZT system in less than 20 min without any loss in diagnostic performance in metastasis staging of high-risk prostate cancer patients.
我们评估了采集时间、能量窗宽度和矩阵大小对全身Tc-HMDP SPECT/CT在前列腺癌原发转移分期中的图像质量、定量分析及诊断性能的影响。
30例前列腺癌患者使用Discovery NM/CT 670 CZT系统进行从头至大腿中部的Tc-HMDP SPECT/CT检查,采用列表模式采集,采集时间为50分钟,能量窗宽度为15%,矩阵大小为128×128。将采集到的列表模式数据重新采样,以生成采集时间分别为41、38、32、26、20和16分钟的数据集,能量窗更窄,分别为10%、8%、6%和4%,以及矩阵大小为256×256的数据集。由三名经验丰富的核医学医师对图像进行定性评估,并通过噪声、病变对比度和SUV测量进行定量评估。由两名经验丰富的核医学医师根据患者、区域和病变水平的敏感性和特异性对诊断性能进行评估。
最初采集的图像具有最佳的定性图像质量和最低的噪声。然而,采集时间可缩短至38分钟,能量窗可窄至8%,矩阵大小可增至256×256,而定性图像质量仍可接受。病变对比度和SUV不受采集参数变化的影响。采集时间的减少对诊断性能没有影响,因为50分钟和缩短采集时间的图像之间的敏感性、特异性、准确性和受试者操作特征曲线下面积没有显著差异。两位阅片者在50分钟、32分钟、26分钟和16分钟图像上的平均患者水平敏感性分别为88%、92%、100%和96%,相应的特异性分别为78%、84%、84%和78%。两位阅片者在50分钟、32分钟、26分钟和16分钟图像上的平均区域水平敏感性分别为55%、58%、59%和56%,相应的特异性分别为95%、98%、96%和95%。随着采集时间的减少,可疑病变的数量趋于增加。
对于高危前列腺癌患者的转移分期,使用通用CZT系统在不到20分钟内即可完成全身Tc-HMDP SPECT/CT检查,且诊断性能不会有任何损失。