Conlon Matthew, Thommen Rachel, Kazim Syed Faraz, Dicpinigaitis Alis J, Schmidt Meic H, McKee Rohini G, Bowers Christian A
School of Medicine, New York Medical College, Valhalla, NY, USA.
Department of Neurosurgery, University of New Mexico Hospital (UNMH), Albuquerque, NM, USA.
Neurospine. 2022 Dec;19(4):1039-1048. doi: 10.14245/ns.2244326.163. Epub 2022 Dec 31.
To assess the discriminative ability of the Risk Analysis Index-administrative (RAI-A) and its recalibrated version (RAI-Rev), compared to the 5-factor modified frailty index (mFI-5), in predicting postoperative outcomes in patients undergoing surgical intervention for traumatic spine injuries (TSIs).
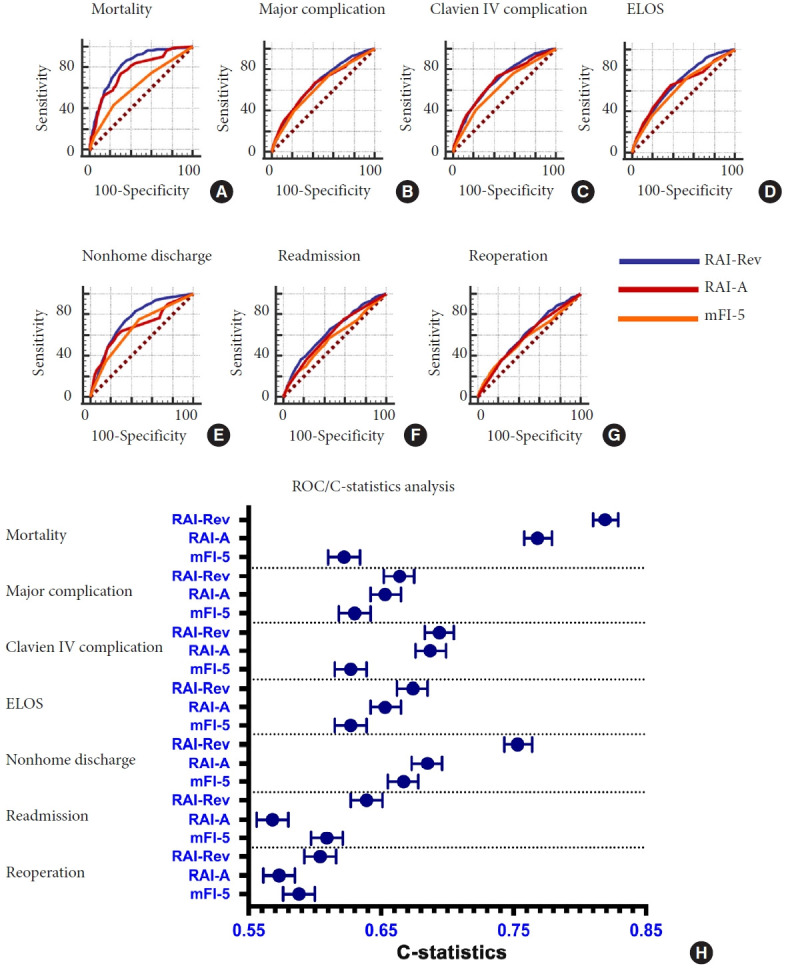
The Current Procedural Terminology (CPT) and International Classification of Disease-9 (ICD-9) and ICD-10 codes were used to identify patients ≥ 18 years who underwent surgical intervention for TSI from National Surgical Quality Improvement Program (ACS-NSQIP) database 2015-2019 (n = 6,571). Multivariate analysis and receiver operating characteristic (ROC) curve analysis were conducted to evaluate the comparative discriminative ability of RAI-Rev, RAI-A, and mFI-5 for 30-day postoperative outcomes.
Multivariate regression analysis showed that with all 3 frailty scores, increasing frailty tiers resulted in worse postoperative outcomes, and patients identified as frail and severely frail using RAI-Rev and RAI-A had the highest odds of poor outcomes. In the ROC curve/C-statistics analysis for prediction of 30-day mortality and morbidity, both RAI-Rev and RAI-A outperformed mFI-5, and for many outcomes, RAI-Rev showed better discriminative performance compared to RAI-A, including mortality (p = 0.0043, DeLong test), extended length of stay (p = 0.0042), readmission (p < 0.0001), reoperation (p = 0.0175), and nonhome discharge (p < 0.0001).
Both RAI-Rev and RAI-A performed better than mFI-5, and RAI-Rev was superior to RAI-A in predicting postoperative mortality and morbidity in TSI patients. RAI-based frailty indices can be used in preoperative risk assessment of spinal trauma patients.
评估风险分析指数-行政版(RAI-A)及其重新校准版本(RAI-Rev)与5因素改良衰弱指数(mFI-5)相比,在预测因创伤性脊柱损伤(TSI)接受手术干预患者术后结局方面的鉴别能力。
使用当前程序编码术语(CPT)以及国际疾病分类第9版(ICD-9)和第10版(ICD-10)编码,从2015 - 2019年国家外科质量改进计划(ACS-NSQIP)数据库中识别≥18岁因TSI接受手术干预的患者(n = 6571)。进行多变量分析和受试者工作特征(ROC)曲线分析,以评估RAI-Rev、RAI-A和mFI-5对术后30天结局的比较鉴别能力。
多变量回归分析表明,对于所有3种衰弱评分,衰弱等级增加会导致术后结局更差,使用RAI-Rev和RAI-A识别为衰弱和严重衰弱的患者不良结局几率最高。在预测30天死亡率和发病率的ROC曲线/C统计分析中,RAI-Rev和RAI-A均优于mFI-5,并且对于许多结局,RAI-Rev与RAI-A相比显示出更好的鉴别性能,包括死亡率(p = 0.0043,德龙检验)、住院时间延长(p = 0.0042)、再入院(p < 0.0001)、再次手术(p = 0.0175)和非回家出院(p < 0.0001)。
RAI-Rev和RAI-A在预测TSI患者术后死亡率和发病率方面均优于mFI-5,且RAI-Rev优于RAI-A。基于RAI-Rev的衰弱指数可用于脊柱创伤患者的术前风险评估。