Digestive and Vascular Center, Department of Pancreatic Surgery, The First Affiliated Hospital of Xinjiang Medical University, Urumqi, 830054, People's Republic of China.
BMC Surg. 2023 Jan 28;23(1):25. doi: 10.1186/s12893-023-01916-9.
The present study aimed to identify risk factors for venous thromboembolism (VTE) after pancreaticoduodenectomy (PD) and to develop and internally validate a predictive model for the risk of venous thrombosis.
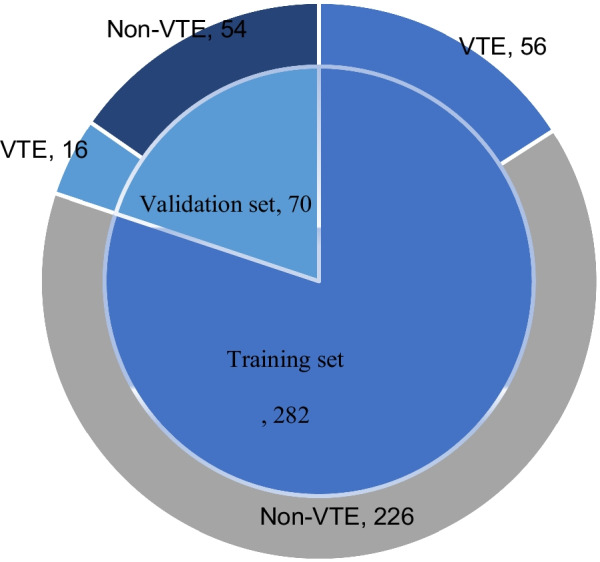
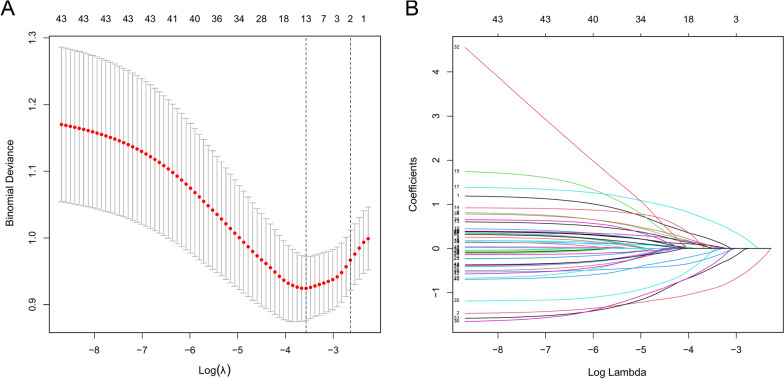
We retrospectively collected data from 352 patients who visited our hospital to undergo PD from January 2018 to March 2022. The number of patients recruited was divided in an 8:2 ratio by using the random split method, with 80% of the patients serving as the training set and 20% as the validation set. The least absolute shrinkage and selection operator (Lasso) regression model was used to optimize feature selection for the VTE risk model. Multivariate logistic regression analysis was used to construct a prediction model by incorporating the features selected in the Lasso model. C-index, receiver operating characteristic curve, calibration plot, and decision curve were used to assess the accuracy of the model, to calibrate the model, and to determine the clinical usefulness of the model. Finally, we evaluated the prediction model for internal validation.
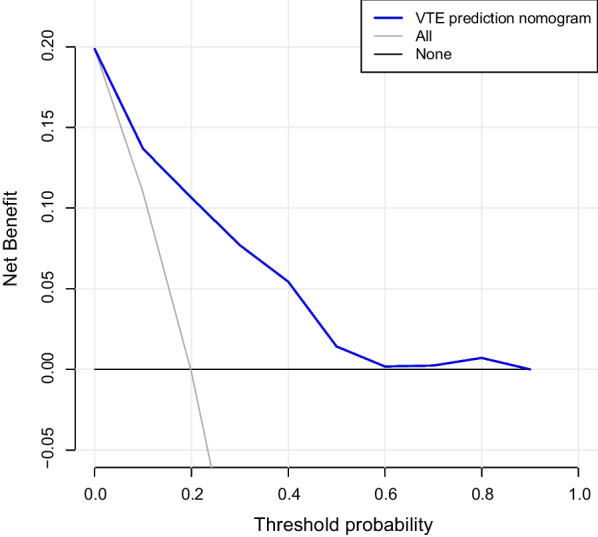
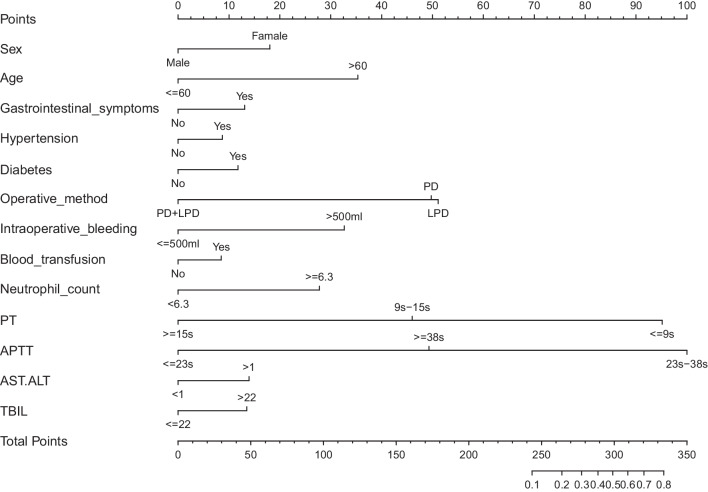
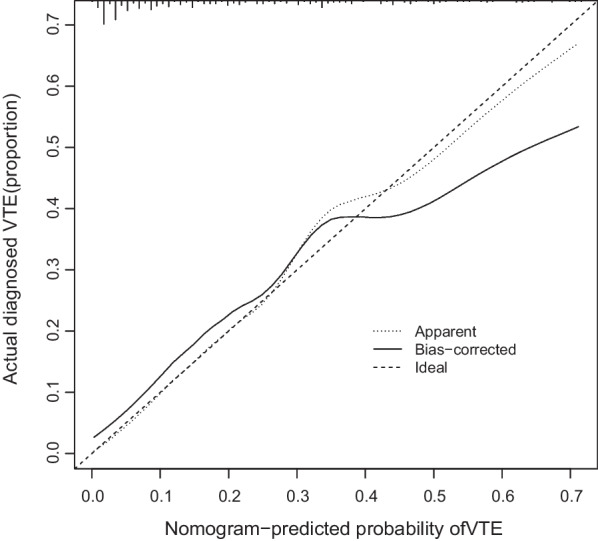
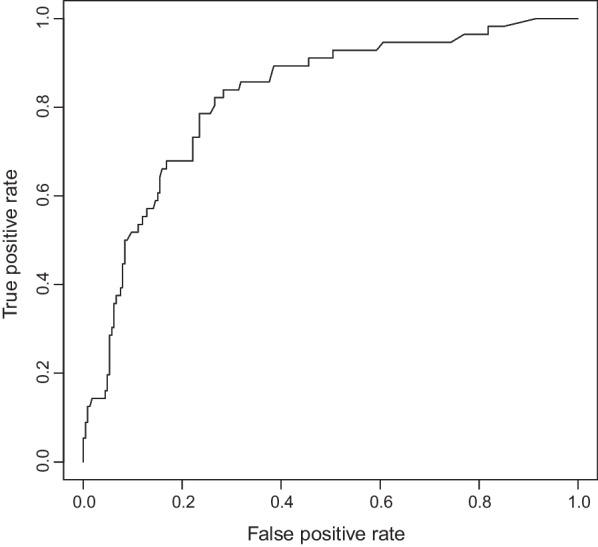
The predictors included in the prediction nomogram were sex, age, gastrointestinal symptoms, hypertension, diabetes, operative method, intraoperative bleeding, blood transfusion, neutrophil count, prothrombin time (PT), activated partial thromboplastin time (APTT), aspartate aminotransferase (AST)/alanine aminotransferase (ALT) ratio (AST/ALT), and total bilirubin (TBIL). The model showed good discrimination with a C-index of 0.827, had good consistency based on the calibration curve, and had an area under the ROC curve value of 0.822 (P < 0.001, 95%confidence interval:0.761-0.882). A high C-index value of 0.894 was reached in internal validation. Decision curve analysis showed that the VTE nomogram was clinically useful when intervention was decided at the VTE possibility threshold of 10%.
The novel model developed in this study is highly targeted and enables personalized assessment of VTE occurrence in patients who undergo PD. The predictors are easily accessible and facilitate the assessment of patients by clinical practitioners.
本研究旨在确定胰十二指肠切除术(PD)后静脉血栓栓塞(VTE)的危险因素,并建立和内部验证静脉血栓形成风险的预测模型。
我们回顾性收集了 2018 年 1 月至 2022 年 3 月期间在我院接受 PD 的 352 名患者的数据。使用随机分割法将患者人数分为 8:2 比例,其中 80%的患者作为训练集,20%作为验证集。最小绝对收缩和选择算子(Lasso)回归模型用于优化 VTE 风险模型的特征选择。使用多变量逻辑回归分析通过包含 Lasso 模型中选择的特征来构建预测模型。C 指数、接收者操作特征曲线、校准图和决策曲线用于评估模型的准确性、校准模型和确定模型的临床实用性。最后,我们评估了内部验证的预测模型。
预测列线图中包含的预测因素包括性别、年龄、胃肠道症状、高血压、糖尿病、手术方法、术中出血、输血、中性粒细胞计数、凝血酶原时间(PT)、活化部分凝血活酶时间(APTT)、天冬氨酸转氨酶/丙氨酸转氨酶(AST/ALT)比值(AST/ALT)和总胆红素(TBIL)。该模型具有良好的区分度,C 指数为 0.827,校准曲线显示出良好的一致性,ROC 曲线下面积值为 0.822(P<0.001,95%置信区间:0.761-0.882)。内部验证中达到了较高的 C 指数值 0.894。决策曲线分析表明,当在 VTE 可能性阈值为 10%时决定干预时,VTE 列线图具有临床实用性。
本研究中开发的新模型具有高度针对性,能够对接受 PD 的患者的 VTE 发生进行个性化评估。预测因素易于获取,便于临床医生对患者进行评估。