Bachtiger Patrik, Kelshiker Mihir A, Petri Camille F, Gandhi Manisha, Shah Moulesh, Kamalati Tahereh, Khan Samir Ali, Hooper Gareth, Stephens Jon, Alrumayh Abdullah, Barton Carys, Kramer Daniel B, Plymen Carla M, Peters Nicholas S
National Heart and Lung Institue, Imperial College London, London, UK.
Imperial College Healthcare NHS Trust, London, UK.
BMJ Health Care Inform. 2023 Mar;30(1). doi: 10.1136/bmjhci-2022-100718.
Most patients with heart failure (HF) are diagnosed following a hospital admission. The clinical and health economic impacts of index HF diagnosis made on admission to hospital versus community settings are not known.
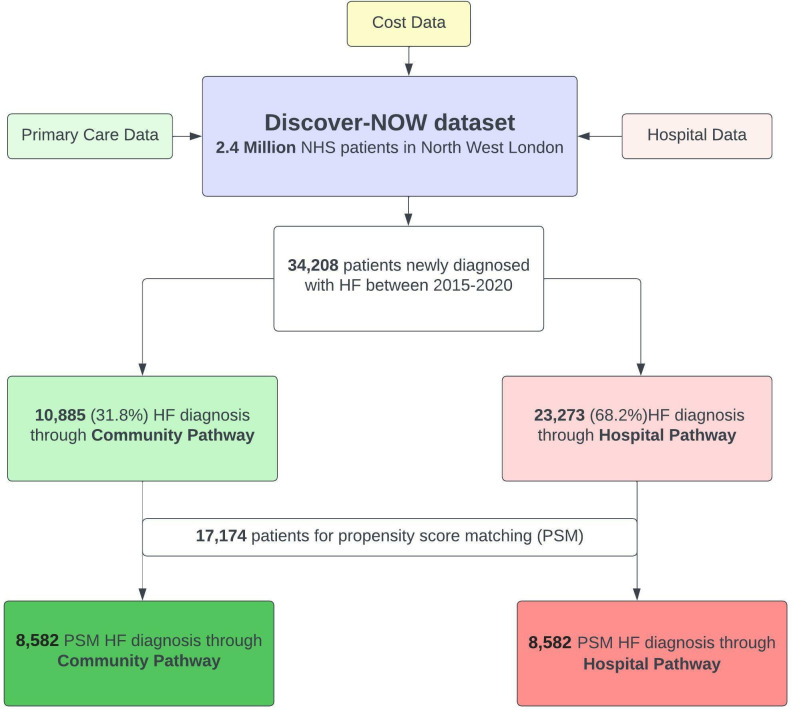
We used the North West London Discover database to examine 34 208 patients receiving an index diagnosis of HF between January 2015 and December 2020. A propensity score-matched (PSM) cohort was identified to adjust for differences in socioeconomic status, cardiovascular risk and pre-diagnosis health resource utilisation cost. Outcomes were stratified by two pathways to index HF diagnosis: a 'hospital pathway' was defined by diagnosis following hospital admission; and a 'community pathway' by diagnosis via a general practitioner or outpatient services. The primary clinical and health economic endpoints were all-cause mortality and cost-consequence differential, respectively.
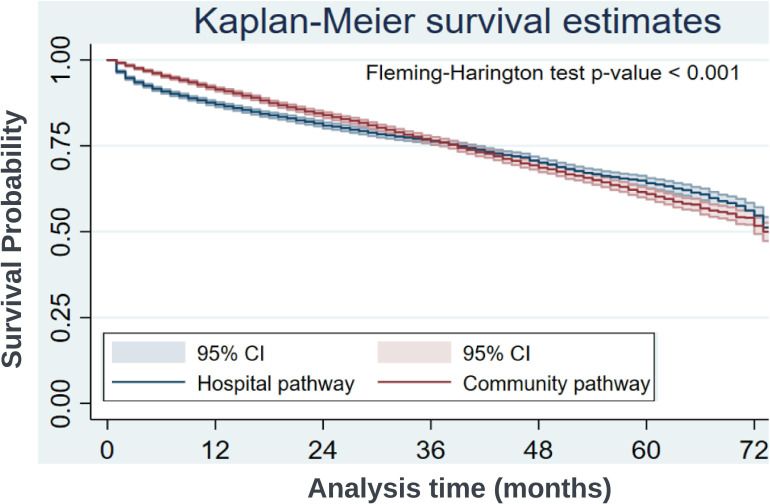
The diagnosis of HF was via hospital pathway in 68% (23 273) of patients. The PSM cohort included 17 174 patients (8582 per group) and was matched across all selected confounders (p>0.05). The ratio of deaths per person-months at 24 months comparing community versus hospital diagnosis was 0.780 (95% CI 0.722 to 0.841, p<0.0001). By 72 months, the ratio of deaths was 0.960 (0.905 to 1.020, p=0.18). Diagnosis via hospital pathway incurred an overall extra longitudinal cost of £2485 per patient.
Index diagnosis of HF through hospital admission continues to dominate and is associated with a significantly greater short-term risk of mortality and substantially increased long-term costs than if first diagnosed in the community. This study highlights the potential for community diagnosis-early, before symptoms necessitate hospitalisation-to improve both clinical and health economic outcomes.
大多数心力衰竭(HF)患者是在住院后被诊断出来的。入院时与社区环境中进行的首次HF诊断对临床和卫生经济的影响尚不清楚。
我们使用伦敦西北部发现数据库,研究了2015年1月至2020年12月期间接受首次HF诊断的34208例患者。通过倾向评分匹配(PSM)队列来调整社会经济地位、心血管风险和诊断前卫生资源利用成本的差异。结果根据首次HF诊断的两种途径进行分层:“医院途径”定义为住院后诊断;“社区途径”定义为通过全科医生或门诊服务诊断。主要临床和卫生经济终点分别是全因死亡率和成本-后果差异。
HF诊断通过医院途径的患者占68%(23273例)。PSM队列包括17174例患者(每组8582例),在所有选定的混杂因素上进行了匹配(p>0.05)。比较社区诊断与医院诊断,24个月时每患者月死亡人数的比率为0.780(95%CI 0.722至0.841,p<0.0001)。到72个月时,死亡比率为0.960(0.905至1.020,p=0.18)。通过医院途径诊断每名患者总体额外产生2485英镑的纵向成本。
通过住院进行HF的首次诊断仍然占主导地位,与社区首次诊断相比,短期死亡风险显著更高,长期成本大幅增加。本研究强调了在症状需要住院治疗之前进行早期社区诊断以改善临床和卫生经济结果的潜力。