National Heart and Lung Institute and Centre for Cardiac Engineering, Imperial College London, London, UK; Imperial College Healthcare NHS Trust, London, UK; UKRI Centre for Doctoral Training in AI for Healthcare, Imperial College London, London, UK.
National Heart and Lung Institute and Centre for Cardiac Engineering, Imperial College London, London, UK; UKRI Centre for Doctoral Training in AI for Healthcare, Imperial College London, London, UK.
Lancet Digit Health. 2022 Feb;4(2):e117-e125. doi: 10.1016/S2589-7500(21)00256-9. Epub 2022 Jan 5.
Most patients who have heart failure with a reduced ejection fraction, when left ventricular ejection fraction (LVEF) is 40% or lower, are diagnosed in hospital. This is despite previous presentations to primary care with symptoms. We aimed to test an artificial intelligence (AI) algorithm applied to a single-lead ECG, recorded during ECG-enabled stethoscope examination, to validate a potential point-of-care screening tool for LVEF of 40% or lower.
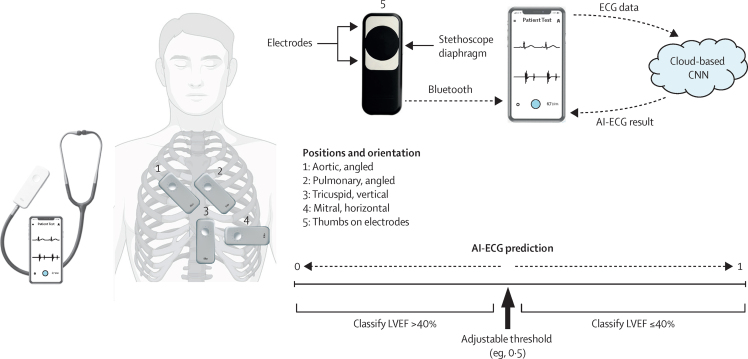
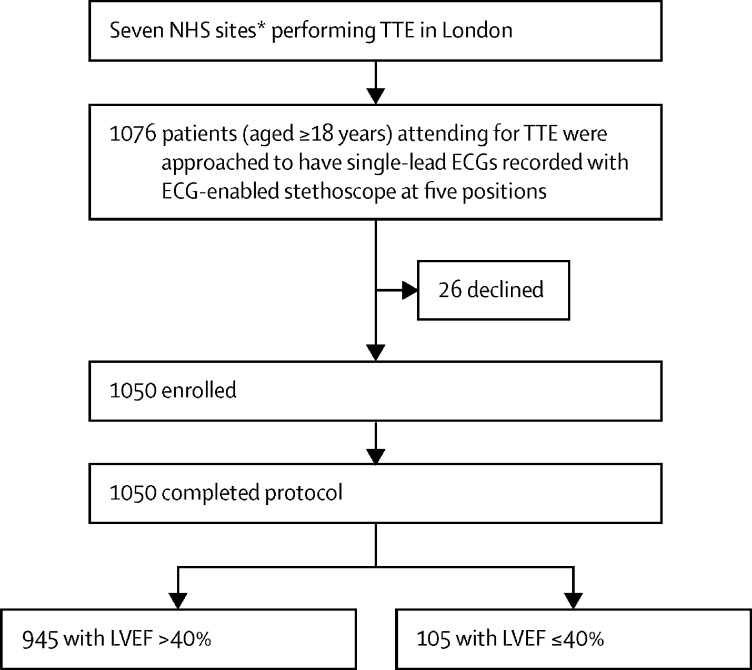
We conducted an observational, prospective, multicentre study of a convolutional neural network (known as AI-ECG) that was previously validated for the detection of reduced LVEF using 12-lead ECG as input. We used AI-ECG retrained to interpret single-lead ECG input alone. Patients (aged ≥18 years) attending for transthoracic echocardiogram in London (UK) were recruited. All participants had 15 s of supine, single-lead ECG recorded at the four standard anatomical positions for cardiac auscultation, plus one handheld position, using an ECG-enabled stethoscope. Transthoracic echocardiogram-derived percentage LVEF was used as ground truth. The primary outcome was performance of AI-ECG at classifying reduced LVEF (LVEF ≤40%), measured using metrics including the area under the receiver operating characteristic curve (AUROC), sensitivity, and specificity, with two-sided 95% CIs. The primary outcome was reported for each position individually and with an optimal combination of AI-ECG outputs (interval range 0-1) from two positions using a rule-based approach and several classification models. This study is registered with ClinicalTrials.gov, NCT04601415.
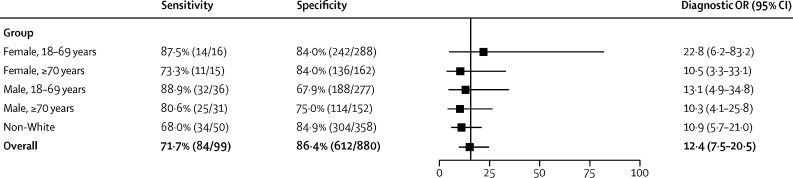
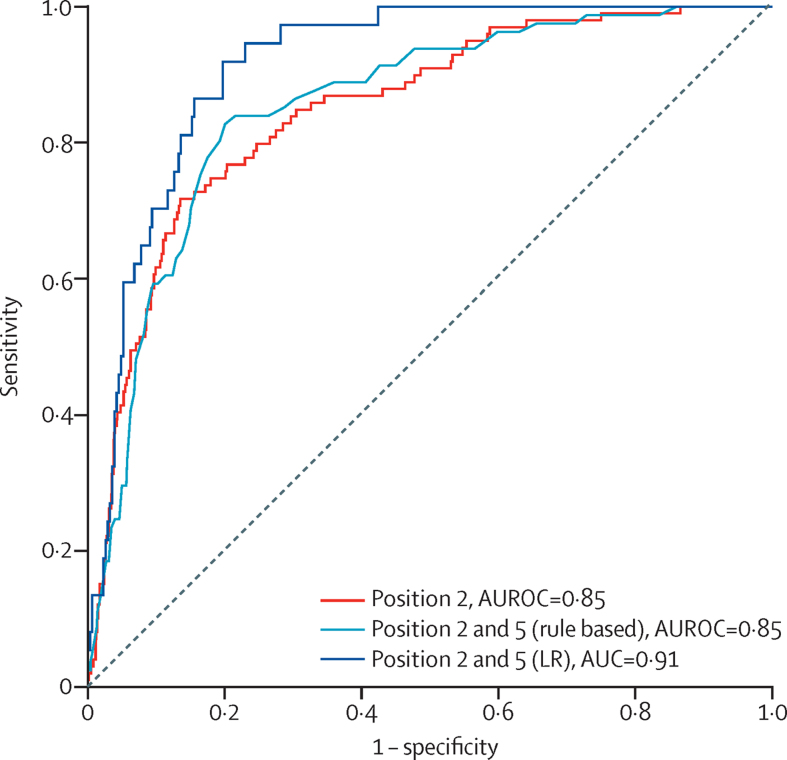
Between Feb 6 and May 27, 2021, we recruited 1050 patients (mean age 62 years [SD 17·4], 535 [51%] male, 432 [41%] non-White). 945 (90%) had an ejection fraction of at least 40%, and 105 (10%) had an ejection fraction of 40% or lower. Across all positions, ECGs were most frequently of adequate quality for AI-ECG interpretation at the pulmonary position (979 [93·3%] of 1050). Quality was lowest for the aortic position (846 [80·6%]). AI-ECG performed best at the pulmonary valve position (p=0·02), with an AUROC of 0·85 (95% CI 0·81-0·89), sensitivity of 84·8% (76·2-91·3), and specificity of 69·5% (66·4-72·6). Diagnostic odds ratios did not differ by age, sex, or non-White ethnicity. Taking the optimal combination of two positions (pulmonary and handheld positions), the rule-based approach resulted in an AUROC of 0·85 (0·81-0·89), sensitivity of 82·7% (72·7-90·2), and specificity of 79·9% (77·0-82·6). Using AI-ECG outputs from these two positions, a weighted logistic regression with l2 regularisation resulted in an AUROC of 0·91 (0·88-0·95), sensitivity of 91·9% (78·1-98·3), and specificity of 80·2% (75·5-84·3).
A deep learning system applied to single-lead ECGs acquired during a routine examination with an ECG-enabled stethoscope can detect LVEF of 40% or lower. These findings highlight the potential for inexpensive, non-invasive, workflow-adapted, point-of-care screening, for earlier diagnosis and prognostically beneficial treatment.
NHS Accelerated Access Collaborative, NHSX, and the National Institute for Health Research.
大多数射血分数降低的心力衰竭患者,当左心室射血分数(LVEF)降至 40%或更低时,在医院被诊断出来。尽管此前在初级保健中出现过症状。我们旨在测试一种应用于单导联心电图的人工智能(AI)算法,该算法是在配备心电图的听诊器检查期间记录的,以验证一种潜在的 40%或更低射血分数的即时护理筛查工具。
我们进行了一项观察性、前瞻性、多中心研究,该研究使用卷积神经网络(称为 AI-ECG),该网络先前已通过使用 12 导联心电图作为输入来检测降低的 LVEF 进行了验证。我们使用经过重新训练的 AI-ECG 来解释单导联心电图输入。在伦敦(英国)接受经胸超声心动图检查的年龄≥18 岁的患者被招募。所有参与者均在仰卧位接受 15 秒的单导联心电图记录,位置为心脏听诊的四个标准解剖位置,外加一个手持位置,使用配备心电图的听诊器。经胸超声心动图衍生的 LVEF 百分比用作地面实况。主要结果是使用包括接收者操作特征曲线(AUROC)下面积在内的指标来衡量 AI-ECG 在分类降低的 LVEF(LVEF ≤40%)方面的性能,敏感性和特异性,置信区间为双侧 95%。主要结果报告了每个位置的性能,以及使用基于规则的方法和几种分类模型从两个位置的 AI-ECG 输出的最佳组合。该研究在 ClinicalTrials.gov 注册,NCT04601415。
在 2021 年 2 月 6 日至 5 月 27 日期间,我们招募了 1050 名患者(平均年龄 62 岁[SD 17.4],535[51%]名男性,432[41%]名非白人)。945(90%)的射血分数至少为 40%,105(10%)的射血分数为 40%或更低。在所有位置中,最常用于 AI-ECG 解释的心电图质量最高的是肺位置(1050 名患者中的 979 名[93.3%])。主动脉位置的质量最低(846[80.6%])。AI-ECG 在肺动脉瓣位置表现最佳(p=0.02),AUROC 为 0.85(0.81-0.89),敏感性为 84.8%(76.2-91.3),特异性为 69.5%(66.4-72.6)。年龄、性别或非白人种族对诊断比值比没有影响。采用两种位置(肺和手持位置)的最佳组合,基于规则的方法导致 AUROC 为 0.85(0.81-0.89),敏感性为 82.7%(72.7-90.2),特异性为 79.9%(77.0-82.6)。使用这两个位置的 AI-ECG 输出,使用 l2 正则化的加权逻辑回归导致 AUROC 为 0.91(0.88-0.95),敏感性为 91.9%(78.1-98.3),特异性为 80.2%(75.5-84.3)。
应用于配备心电图的听诊器在常规检查期间采集的单导联心电图的深度学习系统可以检测到 40%或更低的 LVEF。这些发现突出了用于早期诊断和预后有益治疗的廉价、非侵入性、工作流程适应、即时护理筛查的潜力。
NHS 加速准入协作组织、NHSX 和国家卫生研究院。