Department of Cardiology, Amsterdam UMC Location Vrije Universiteit, Amsterdam, The Netherlands.
The Netherlands Heart Institute, Utrecht, The Netherlands.
Med Princ Pract. 2023;32(3):200-208. doi: 10.1159/000529863. Epub 2023 Mar 22.
The aim of this work was to study sex differences in major bleeding risk in relation to dual antiplatelet therapy (DAPT) after percutaneous coronary intervention (PCI) for acute coronary syndrome (ACS).
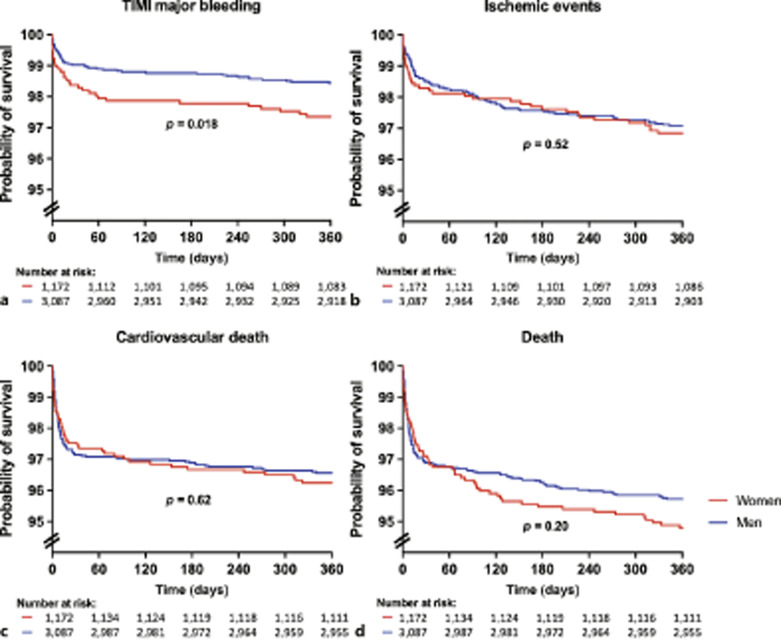
The Rijnmond Collective Cardiology Research registry was designed to evaluate the application and outcomes of DAPT after ACS/PCI in the Rijnmond region in the Netherlands. Overall, 1,172 women (median age 67.5 years) and 3,087 men (median age 62.2 years) with ACS/PCI were enrolled between August 2011 and June 2013. Based on a tailored regional DAPT guideline aiming at bleeding risk minimization, 52.6% women and 66.9% men received prasugrel as first-choice P2Y12 inhibitor, in addition to aspirin. Women more frequently had contraindications for the use of prasugrel (and therefore received clopidogrel) than men (47.9 vs. 26.9%, p < 0.001). Femoral access was more common in women than in men (47.6 vs. 38.1%, p < 0.001). Women had higher incidence of major bleeding at 1 year than men (2.6 vs. 1.6%, p = 0.018). After adjustment for established bleeding risk factors, female sex was associated with over two-fold higher risk of major bleeding (adjusted hazard ratio 2.33; 95% confidence interval 1.26-4.32). This difference was apparent at discharge and appeared to be caused by access site bleedings (0.9 vs. 0.1%, p < 0.001). No sex differences were found in non-access site-related major bleeding up to 1 year.
Women with ACS/PCI receiving DAPT had higher major bleeding risk caused by an excess in access site bleeds, mainly in relation to the femoral approach.
本研究旨在探讨急性冠状动脉综合征(ACS)经皮冠状动脉介入治疗(PCI)后双联抗血小板治疗(DAPT)中女性大出血风险的性别差异。
Rijnmond 联合心脏病学研究注册处旨在评估荷兰 Rijnmond 地区 ACS/PCI 后 DAPT 的应用和结果。共有 1172 名女性(中位年龄 67.5 岁)和 3087 名男性(中位年龄 62.2 岁)因 ACS/PCI 入组,时间为 2011 年 8 月至 2013 年 6 月。基于旨在降低出血风险的个体化区域 DAPT 指南,52.6%的女性和 66.9%的男性接受普拉格雷作为首选 P2Y12 抑制剂,联合阿司匹林。与男性相比,女性使用普拉格雷的禁忌证更常见(47.9% vs. 26.9%,p < 0.001)。与男性相比,女性更常采用股动脉入路(47.6% vs. 38.1%,p < 0.001)。女性 1 年时大出血发生率高于男性(2.6% vs. 1.6%,p = 0.018)。在校正了已知出血风险因素后,女性性别与大出血风险增加两倍以上相关(校正后危险比 2.33;95%置信区间 1.26-4.32)。这种差异在出院时就很明显,并且似乎是由入路部位出血引起的(0.9% vs. 0.1%,p < 0.001)。在 1 年时,未观察到与非入路部位相关的大出血存在性别差异。
接受 DAPT 的 ACS/PCI 女性大出血风险较高,这主要与股动脉入路相关的入路部位出血过多有关。