Cowdrick Kyle R, Urner Tara, Sathialingam Eashani, Fang Zhou, Quadri Ayesha, Turrentine Katherine, Yup Lee Seung, Buckley Erin M
Georgia Institute of Technology and Emory University, Wallace H. Coulter Department of Biomedical Engineering, Atlanta, Georgia, United States.
Children's Healthcare of Atlanta and Emory University School of Medicine, Department of Pediatrics, Atlanta, Georgia, United States.
Neurophotonics. 2023 Apr;10(2):025002. doi: 10.1117/1.NPh.10.2.025002. Epub 2023 Apr 7.
Cerebrovascular reactivity (CVR), i.e., the ability of cerebral vasculature to dilate or constrict in response to vasoactive stimuli, is a biomarker of vascular health. Exogenous administration of inhaled carbon dioxide, i.e., hypercapnia (HC), remains the "gold-standard" intervention to assess CVR. More tolerable paradigms that enable CVR quantification when HC is difficult/contraindicated have been proposed. However, because these paradigms feature mechanistic differences in action, an assessment of agreement of these more tolerable paradigms to HC is needed.
We aim to determine the agreement of CVR assessed during HC, breath-hold (BH), and resting state (RS) paradigms.
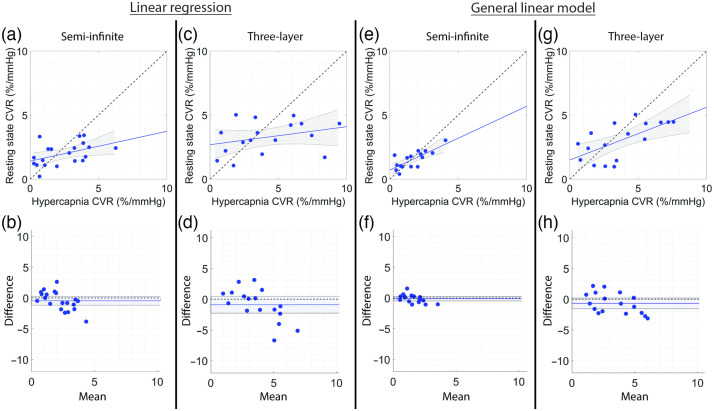
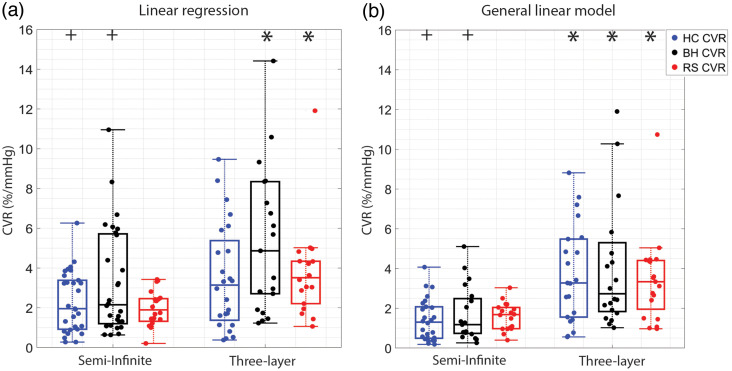
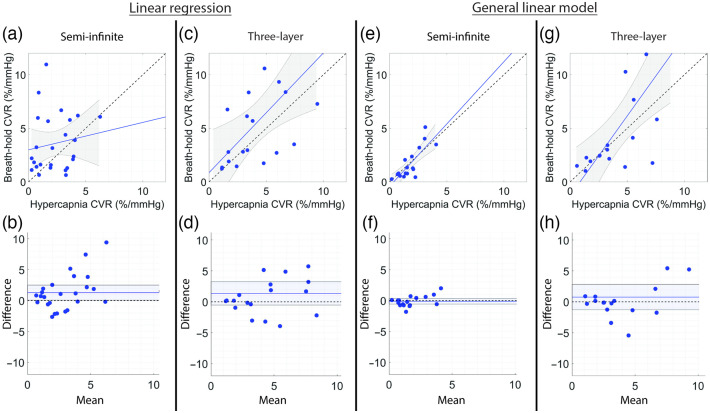
Healthy adults were subject to HC, BH, and RS paradigms. End tidal carbon dioxide (EtCO) and cerebral blood flow (CBF, assessed with diffuse correlation spectroscopy) were monitored continuously. CVR (%/mmHg) was quantified via linear regression of CBF versus EtCO or via a general linear model (GLM) that was used to minimize the influence of systemic and extracerebral signal contributions.
Strong agreement ( ; ) among CVR paradigms was demonstrated when utilizing a GLM to regress out systemic/extracerebral signal contributions. Linear regression alone showed poor agreement across paradigms ( ; ).
More tolerable experimental paradigms coupled with regression of systemic/extracerebral signal contributions may offer a viable alternative to HC for assessing CVR.
脑血管反应性(CVR),即脑血管系统对血管活性刺激作出扩张或收缩反应的能力,是血管健康的生物标志物。吸入二氧化碳的外源给药,即高碳酸血症(HC),仍然是评估CVR的“金标准”干预措施。已经提出了在HC困难/禁忌时能够进行CVR量化的更可耐受的范式。然而,由于这些范式在作用机制上存在差异,因此需要评估这些更可耐受的范式与HC的一致性。
我们旨在确定在HC、屏气(BH)和静息状态(RS)范式期间评估的CVR的一致性。
健康成年人接受HC、BH和RS范式。连续监测呼气末二氧化碳(EtCO)和脑血流量(CBF,用扩散相关光谱法评估)。CVR(%/mmHg)通过CBF与EtCO的线性回归或通过用于最小化全身和脑外信号贡献影响的一般线性模型(GLM)进行量化。
当使用GLM回归全身/脑外信号贡献时,CVR范式之间表现出高度一致性( ; )。单独的线性回归在各范式之间显示出较差的一致性( ; )。
更可耐受的实验范式与全身/脑外信号贡献的回归相结合,可能为评估CVR提供一种可行的替代HC的方法。