Department of Biomedical Data Science, Stanford University School of Medicine, 1265 Welch Road, Stanford, CA, 94305, USA.
Department of Electrical and Computer Engineering, University of North Carolina at Charlotte, 9201 University City Boulevard, Charlotte, NC, 28223, USA.
Sci Rep. 2023 Apr 13;13(1):6047. doi: 10.1038/s41598-023-33365-y.
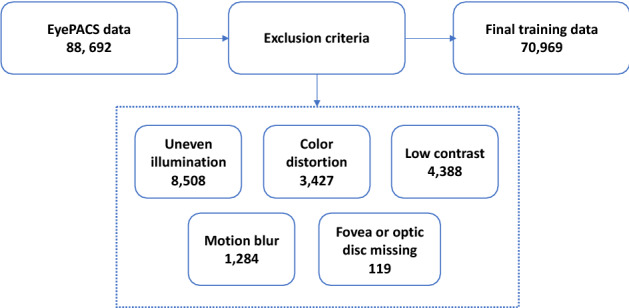
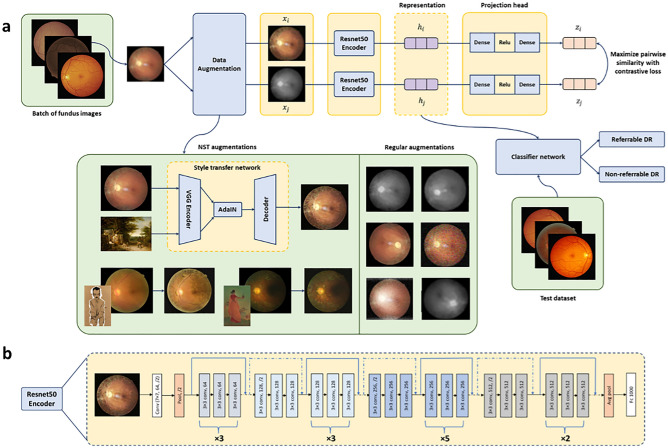
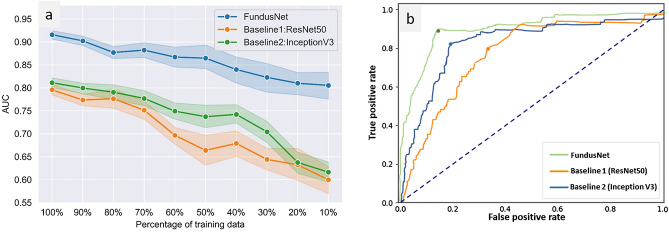
Diabetic retinopathy (DR) is a major cause of vision impairment in diabetic patients worldwide. Due to its prevalence, early clinical diagnosis is essential to improve treatment management of DR patients. Despite recent demonstration of successful machine learning (ML) models for automated DR detection, there is a significant clinical need for robust models that can be trained with smaller cohorts of dataset and still perform with high diagnostic accuracy in independent clinical datasets (i.e., high model generalizability). Towards this need, we have developed a self-supervised contrastive learning (CL) based pipeline for classification of referable vs non-referable DR. Self-supervised CL based pretraining allows enhanced data representation, therefore, the development of robust and generalized deep learning (DL) models, even with small, labeled datasets. We have integrated a neural style transfer (NST) augmentation in the CL pipeline to produce models with better representations and initializations for the detection of DR in color fundus images. We compare our CL pretrained model performance with two state of the art baseline models pretrained with Imagenet weights. We further investigate the model performance with reduced labeled training data (down to 10 percent) to test the robustness of the model when trained with small, labeled datasets. The model is trained and validated on the EyePACS dataset and tested independently on clinical datasets from the University of Illinois, Chicago (UIC). Compared to baseline models, our CL pretrained FundusNet model had higher area under the receiver operating characteristics (ROC) curve (AUC) (CI) values (0.91 (0.898 to 0.930) vs 0.80 (0.783 to 0.820) and 0.83 (0.801 to 0.853) on UIC data). At 10 percent labeled training data, the FundusNet AUC was 0.81 (0.78 to 0.84) vs 0.58 (0.56 to 0.64) and 0.63 (0.60 to 0.66) in baseline models, when tested on the UIC dataset. CL based pretraining with NST significantly improves DL classification performance, helps the model generalize well (transferable from EyePACS to UIC data), and allows training with small, annotated datasets, therefore reducing ground truth annotation burden of the clinicians.
糖尿病性视网膜病变(DR)是全球糖尿病患者视力损害的主要原因。由于其普遍性,早期临床诊断对于改善 DR 患者的治疗管理至关重要。尽管最近已经证明了用于自动 DR 检测的机器学习(ML)模型的成功,但仍然需要稳健的模型,这些模型可以用较小的数据集进行训练,并在独立的临床数据集(即高模型通用性)中仍然具有高诊断准确性。针对这一需求,我们开发了一种基于自监督对比学习(CL)的分类管道,用于分类可转诊与不可转诊的 DR。基于自监督 CL 的预训练允许增强数据表示,因此,即使使用较小的标记数据集,也可以开发稳健且通用的深度学习(DL)模型。我们在 CL 管道中集成了神经风格转换(NST)增强功能,以生成具有更好表示和初始化的模型,用于检测彩色眼底图像中的 DR。我们将我们的 CL 预训练模型的性能与两个使用 Imagenet 权重预训练的最先进基线模型的性能进行了比较。我们还使用减少的标记训练数据(低至 10%)进一步研究了模型性能,以测试模型在使用小的标记数据集进行训练时的鲁棒性。该模型在 EyePACS 数据集上进行训练和验证,并在伊利诺伊大学芝加哥分校(UIC)的临床数据集上独立进行测试。与基线模型相比,我们的 CL 预训练的 FundusNet 模型在 UIC 数据上具有更高的接收器操作特征(ROC)曲线下面积(AUC)(CI)值(0.91(0.898 至 0.930)比 0.80(0.783 至 0.820)和 0.83(0.801 至 0.853))。在标记训练数据低至 10%时,当在 UIC 数据集上进行测试时,FundusNet 的 AUC 为 0.81(0.78 至 0.84),而基线模型为 0.58(0.56 至 0.64)和 0.63(0.60 至 0.66)。基于 NST 的 CL 预训练显著提高了 DL 分类性能,有助于模型很好地泛化(从 EyePACS 转移到 UIC 数据),并且允许使用小的、有注释的数据集进行训练,从而减少了临床医生的真实注释负担。