Yacobson Irina, Wanga Valentine, Ahmed Khatija, Chipato Tsungai, Gichangi Peter, Kiarie James, Louw Cheryl, Morrison Susan, Moss Margaret, Mugo Nelly R, Palanee-Phillips Thesla, Pleaner Melanie, Scoville Caitlin W, Thomas Katherine K, Nanda Kavita
FHI 360, Durham, NC, United States.
Department of Global Health, University of Washington, Seattle, WA, United States.
Contracept X. 2023 Mar 30;5:100092. doi: 10.1016/j.conx.2023.100092. eCollection 2023.
To assess the rates of failed insertion, expulsion, and perforation when intrauterine device (IUD) insertions were done by newly trained clinicians, and to examine factors that may affect these outcomes.
We evaluated skill-based outcomes following IUD insertion at 12 African sites in a secondary analysis of the Evidence for Contraceptive Options and HIV Outcomes (ECHO) randomized trial. Before trial initiation, we provided competency-based IUD training to clinicians and offered ongoing clinical support. We used Cox proportional hazards regression to examine factors associated with expulsion.
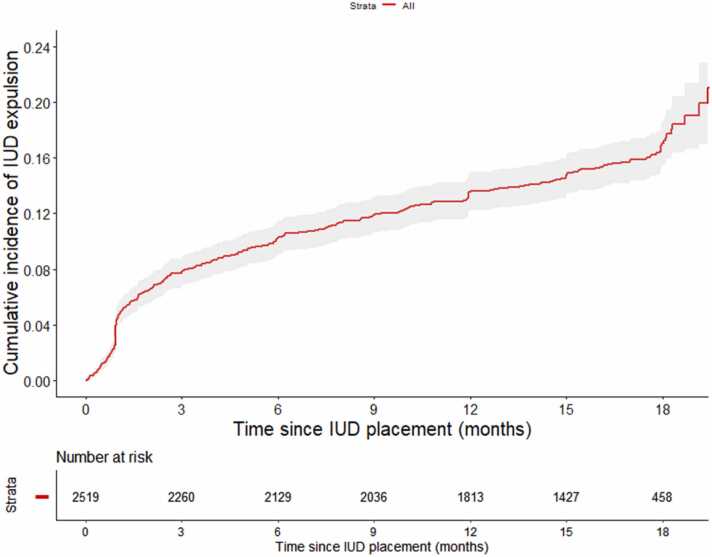
Among 2582 IUD acceptors who underwent first attempted IUD insertion, 141 experienced insertion failure (5.46%) and seven had uterine perforation (0.27%). Perforation was more common among breastfeeding women within three months postpartum (0.65%) compared with non-breastfeeding women (0.22%). We recorded 493 expulsions (15.5 per 100 person-years, 95% confidence interval [CI] 14.1─16.9): 383 partial and 110 complete. The risk of IUD expulsion was lower among women older than 24 years (aHR 0.63, 95% CI 0.50─0.78) and may be higher among nulliparous women. (aHR 1.65, 95% CI 0.97─2.82). Breastfeeding (aHR 0.94, 95% CI 0.72─1.22) had no significant effect on expulsion. IUD expulsion rate was highest during the first three months of the trial.
IUD insertion failure and uterine perforation rates in our study were comparable to those reported in the literature. These results suggest that training, ongoing support, and opportunities to apply new skills were effective in ensuring good clinical outcomes for women receiving IUD insertion by newly trained providers.
Data from this study support recommendations to program managers, policymakers, and clinicians that IUDs can be inserted safely in resource-constrained settings when providers receive appropriate training and support.
评估新培训的临床医生进行宫内节育器(IUD)插入时的插入失败、排出和穿孔率,并检查可能影响这些结果的因素。
在避孕选择与HIV结局证据(ECHO)随机试验的二次分析中,我们评估了12个非洲地点IUD插入后的基于技能的结局。在试验开始前,我们为临床医生提供了基于能力的IUD培训,并提供持续的临床支持。我们使用Cox比例风险回归来检查与排出相关的因素。
在2582名首次尝试插入IUD的接受者中,141人经历了插入失败(5.46%),7人发生子宫穿孔(0.27%)。与非哺乳期妇女(0.22%)相比,产后三个月内的哺乳期妇女穿孔更为常见(0.65%)。我们记录了493次排出(每100人年15.5次,95%置信区间[CI]14.1─16.9):383次部分排出和110次完全排出。24岁以上女性的IUD排出风险较低(校正风险比[aHR]0.63,95%CI 0.50─0.78),未生育女性的排出风险可能较高(aHR 1.65,95%CI 0.97─2.82)。母乳喂养(aHR 0.94,95%CI 0.72─1.22)对排出无显著影响。IUD排出率在试验的前三个月最高。
我们研究中的IUD插入失败率和子宫穿孔率与文献报道的相当。这些结果表明,培训、持续支持以及应用新技能的机会对于确保新培训的提供者为接受IUD插入的女性取得良好临床结局是有效的。
本研究的数据支持向项目管理者、政策制定者和临床医生提出的建议,即当提供者接受适当培训和支持时,IUD可在资源有限的环境中安全插入。