Thomas Deena, Sharma Akash, Sankar M Jeeva
Department of Pediatrics, Muthoot Hospitals, Kozhencherry, Kerala, India.
Department of Pediatrics, Sir Padampat Institute of Neonatology and Pediatric Health (SPINPH), SMS Medical College, Jaipur, India.
Front Nutr. 2023 Jun 14;10:1133293. doi: 10.3389/fnut.2023.1133293. eCollection 2023.
Probiotics have been shown to reduce the risk of mortality and necrotizing enterocolitis (NEC) in very low birth weight (VLBW) neonates. The probiotic species with the maximal benefits in neonates from low- and middle-income countries are unknown.
To identify the strain of probiotics with the maximum benefit in preventing neonatal mortality, sepsis, and NEC using the Bayesian network meta-analysis.
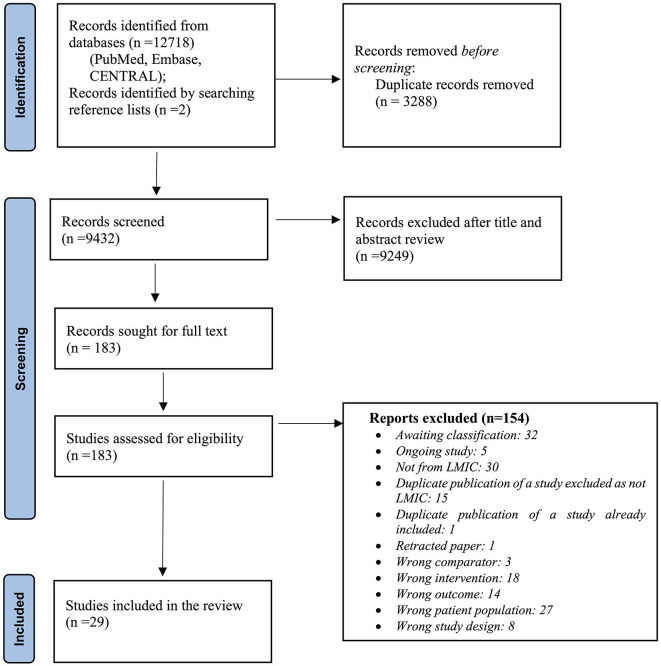
We searched Medline via PubMed, Embase, and Cochrane Central Register of Controlled Trials (CENTRAL). We also hand-searched reference lists of previous systematic reviews to identify eligible studies.
Randomized controlled trials (RCTs) from LMICs comparing enteral supplementation of one or more probiotics with another probiotic species or placebo were included.
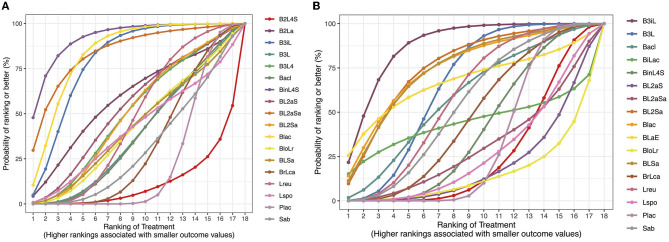
Two authors screened the studies, extracted the data, and examined the risk of bias using the Cochrane risk of bias 2 (RoB 2) tools. Bayesian network meta-analysis was performed using the "BUGSnet" package in R and RStudio (version 1.4.1103). The confidence in the findings was assessed using the Confidence in Network Meta-analysis (CINeMA) web application.
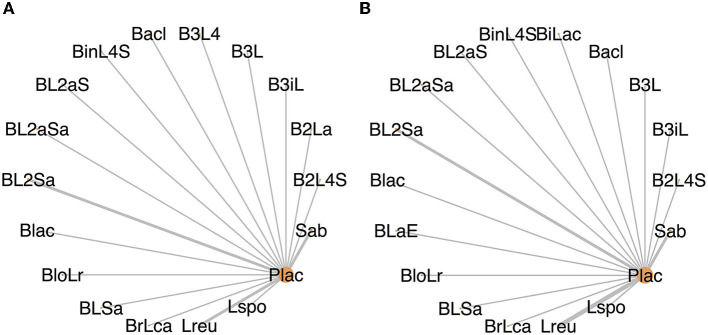
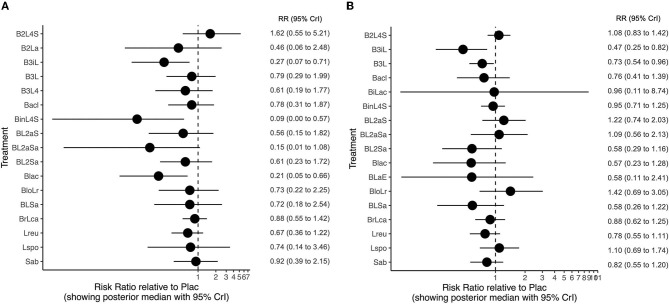
Twenty-nine RCTs enrolling 4,906 neonates and evaluating 24 probiotics were included. Only 11 (38%) studies had a low risk of bias. All the studies compared the probiotics with a placebo; none had a head-to-head comparison of different probiotic species. Also, only one study each had evaluated most probiotic regimens. When compared to placebo, the combination of , and may reduce the risk of mortality (relative risk [RR] 0.26; 95% credible interval [CrI] 0.07 to 0.72), sepsis (RR 0.47; 95% CrI 0.25 to 0.83), and NEC (RR 0.31; 95% CrI 0.10 to 0.78) but the evidence is very uncertain. There is low certainty evidence that the single probiotic species, , could reduce the risk of mortality (RR 0.21; 0.05 to 0.66) and NEC (RR 0.09; 0.01 to 0.32).
Given the low to very low certainty of evidence for the efficacy of the two probiotics found to reduce mortality and necrotizing enterocolitis, no firm conclusions can be made on the optimal probiotics for use in preterm neonates in low- and middle-income countries.
https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022353242, identifier: CRD42022353242.
已证明益生菌可降低极低出生体重(VLBW)新生儿的死亡率和坏死性小肠结肠炎(NEC)风险。在低收入和中等收入国家的新生儿中,具有最大益处的益生菌种类尚不清楚。
使用贝叶斯网络荟萃分析确定在预防新生儿死亡、败血症和NEC方面具有最大益处的益生菌菌株。
我们通过PubMed、Embase和Cochrane对照试验中央注册库(CENTRAL)检索了Medline。我们还手工检索了先前系统评价的参考文献列表,以确定符合条件的研究。
纳入来自低收入和中等收入国家的随机对照试验(RCT),这些试验比较了一种或多种益生菌与另一种益生菌或安慰剂的肠内补充情况。
两位作者筛选了研究,提取了数据,并使用Cochrane偏倚风险2(RoB 2)工具检查了偏倚风险。使用R和RStudio(版本1.4.1103)中的“BUGSnet”软件包进行贝叶斯网络荟萃分析。使用网络荟萃分析置信度(CINeMA)网络应用程序评估研究结果的可信度。
纳入了29项RCT,共4906名新生儿,评估了24种益生菌。只有11项(38%)研究的偏倚风险较低。所有研究均将益生菌与安慰剂进行了比较;没有对不同益生菌种类进行直接比较。此外,每种益生菌方案大多仅在一项研究中进行了评估。与安慰剂相比,[具体益生菌种类1]、[具体益生菌种类2]和[具体益生菌种类3]的组合可能会降低死亡率(相对风险[RR] 0.26;95%可信区间[CrI] 0.07至0.72)、败血症(RR 0.47;95% CrI 0.25至0.83)和NEC(RR 0.31;95% CrI 0.10至0.78)的风险,但证据非常不确定。有低确定性证据表明单一益生菌种类[具体益生菌种类4]可降低死亡率(RR 0.21;0.05至0.66)和NEC(RR 0.09;0.01至0.32)的风险。
鉴于所发现的两种益生菌降低死亡率和坏死性小肠结肠炎疗效的证据确定性低至极低,对于低收入和中等收入国家早产儿使用的最佳益生菌无法得出确切结论。
https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022353242,标识符:CRD42022353242。