Department of Anaesthesia and Intensive Care, The Chinese University of Hong Kong, Hong Kong SAR, China.
The Jockey Club School of Public Health and Primary Care, The Chinese University of Hong Kong, Hong Kong SAR, China.
BMJ Open. 2023 Jul 10;13(7):e067101. doi: 10.1136/bmjopen-2022-067101.
Direct comparisons between COVID-19 and influenza A in the critical care setting are limited. The objective of this study was to compare their outcomes and identify risk factors for hospital mortality.
This was a territory-wide, retrospective study on all adult (≥18 years old) patients admitted to public hospital intensive care units in Hong Kong. We compared COVID-19 patients admitted between 27 January 2020 and 26 January 2021 with a propensity-matched historical cohort of influenza A patients admitted between 27 January 2015 and 26 January 2020. We reported outcomes of hospital mortality and time to death or discharge. Multivariate analysis using Poisson regression and relative risk (RR) was used to identify risk factors for hospital mortality.
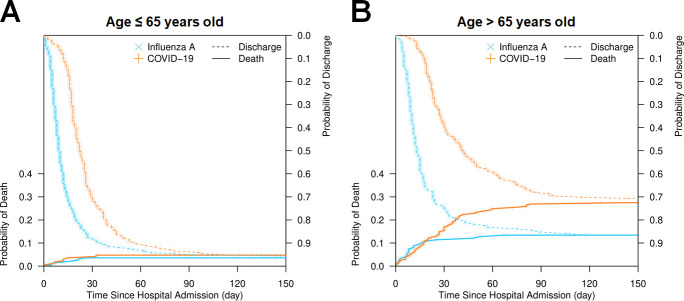
After propensity matching, 373 COVID-19 and 373 influenza A patients were evenly matched for baseline characteristics. COVID-19 patients had higher unadjusted hospital mortality than influenza A patients (17.5% vs 7.5%, p<0.001). The Acute Physiology and Chronic Health Evaluation IV (APACHE IV) adjusted standardised mortality ratio was also higher for COVID-19 than influenza A patients ((0.79 (95% CI 0.61 to 1.00) vs 0.42 (95% CI 0.28 to 0.60)), p<0.001). Adjusting for age, PO/FO, Charlson Comorbidity Index and APACHE IV, COVID-19 (adjusted RR 2.26 (95% CI 1.52 to 3.36)) and early bacterial-viral coinfection (adjusted RR 1.66 (95% CI 1.17 to 2.37)) were directly associated with hospital mortality.
Critically ill patients with COVID-19 had substantially higher hospital mortality when compared with propensity-matched patients with influenza A.
在重症监护环境中,COVID-19 与甲型流感之间的直接比较有限。本研究的目的是比较它们的结果并确定医院死亡率的危险因素。
这是一项全港性的回顾性研究,纳入了香港公立医院重症监护病房所有成年(≥18 岁)患者。我们将 2020 年 1 月 27 日至 2021 年 1 月 26 日期间收治的 COVID-19 患者与 2015 年 1 月 27 日至 2020 年 1 月 26 日期间收治的甲型流感患者进行了倾向性匹配的历史队列进行比较。我们报告了医院死亡率和死亡或出院时间的结果。使用泊松回归和相对风险(RR)的多变量分析来确定医院死亡率的危险因素。
经过倾向性匹配后,373 例 COVID-19 和 373 例甲型流感患者的基线特征均衡匹配。COVID-19 患者的未调整医院死亡率高于甲型流感患者(17.5%比 7.5%,p<0.001)。COVID-19 患者的急性生理学和慢性健康评估 IV(APACHE IV)调整后的标准化死亡率比值也高于甲型流感患者((0.79(95%CI 0.61 至 1.00)比 0.42(95%CI 0.28 至 0.60)),p<0.001)。在校正年龄、PO/FO、Charlson 合并症指数和 APACHE IV 后,COVID-19(校正 RR 2.26(95%CI 1.52 至 3.36))和早期细菌-病毒合并感染(校正 RR 1.66(95%CI 1.17 至 2.37))与医院死亡率直接相关。
与甲型流感倾向性匹配患者相比,COVID-19 重症患者的医院死亡率显著更高。