Cicely Saunders Institute of Palliative Care, Policy, and Rehabilitation, King's College London, London, United Kingdom.
GKT School of Medical Education, King's College London, London, United Kingdom.
Front Public Health. 2023 Jul 26;11:1180571. doi: 10.3389/fpubh.2023.1180571. eCollection 2023.
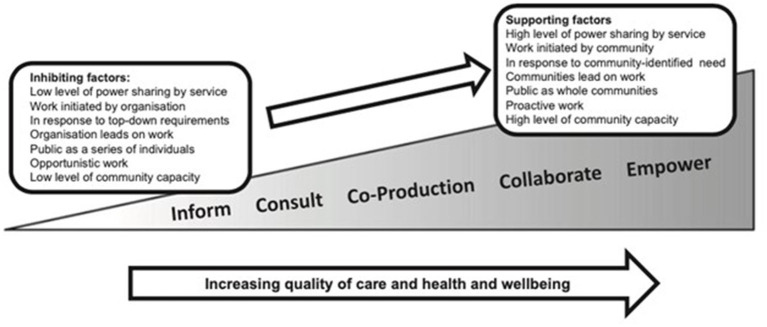
Public health palliative care views communities as an integral part of care delivery at the end of life. This community-provider partnership approach has the potential to improve end-of-life care for people who are dying and their carers.
To identify and appraise the current literature related to public health interventions that enable communities to support people who are dying and their carers.
A scoping review was conducted, applying Arksey and O'Malley's methods. Data was extracted and synthesized using narrative techniques, and results are reported using PRISMA guidelines.
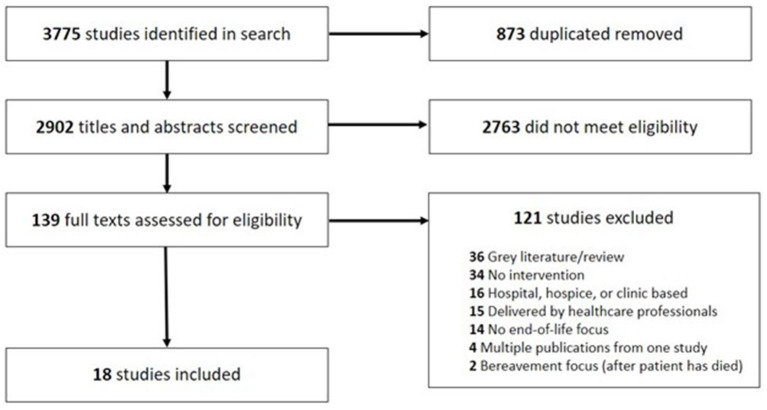
The search yielded 2,902 results. Eighteen met inclusion criteria and were included in the analysis. Interventions were categorized according to their target population: people with life-limiting illness (ex. facilitated social interaction, helplines and guided discussions about death and dying); carers (ex. social support mapping, psychoeducation, and community resource identification and facilitation); or dyads (ex. reminiscence activities, practical and emotional support from volunteers, online modules to bolster coping mechanisms). Public health palliative care approaches were delivered by key community stakeholders such as community health workers, volunteers, peer mentors, and pre-established support groups. Despite reported challenges in identifying appropriate tools to measure effectiveness, studies report improvement in quality of life, loneliness, social support, stress and self-efficacy.
We found that community-engaged palliative care interventions can lead to appreciable changes in various outcomes, though it was difficult to determine in which contexts this approach works best because of the dearth of contextual information reported. Based on the varied design and implementation strategies, it is clear that no one method for enhancing end of life care will benefit all communities and it is crucial to engage community members at all stages of the design and implementation process. Future research should be grounded in appropriate theory, describe contextual differences in these communities, and should specifically examine how demographics, resource availability, and social capital might impact the design, implementation, and results of public health palliative care interventions.
公共卫生姑息治疗将社区视为生命终末期护理服务的一个组成部分。这种社区-提供者合作方法有可能改善临终患者及其照护者的临终关怀。
确定并评价与公共卫生干预措施相关的现有文献,这些干预措施使社区能够支持临终患者及其照护者。
采用阿特金和奥马利的方法进行了范围综述。使用叙述性技术提取和综合数据,并按照 PRISMA 指南报告结果。
搜索结果为 2902 条。符合纳入标准的有 18 项,纳入分析。干预措施根据其目标人群进行分类:患有绝症的人(例如促进社交互动、热线和关于死亡和濒死的引导讨论);照护者(例如社会支持绘图、心理教育以及社区资源识别和促进);或二人组(例如回忆活动、志愿者提供的实际和情感支持、增强应对机制的在线模块)。公共卫生姑息治疗方法由关键的社区利益相关者提供,如社区卫生工作者、志愿者、朋辈导师和预先建立的支持小组。尽管在确定适当的工具来衡量效果方面存在挑战,但研究报告显示生活质量、孤独感、社会支持、压力和自我效能感有所改善。
我们发现,社区参与的姑息治疗干预措施可以导致各种结果的显著变化,尽管由于报告的背景信息不足,难以确定这种方法在哪些情况下效果最好。基于不同的设计和实施策略,显然没有一种方法可以使所有社区都受益于改善临终关怀,因此在设计和实施过程的各个阶段都必须让社区成员参与进来。未来的研究应基于适当的理论,描述这些社区的背景差异,并特别研究人口统计学、资源可用性和社会资本如何可能影响公共卫生姑息治疗干预措施的设计、实施和结果。