Hippisley-Cox Julia, Mei Winnie, Fitzgerald Rebecca, Coupland Carol
Nuffield Department of Primary Health Care Sciences, University of Oxford, England.
Early Cancer Institute, University of Cambridge and Addenbrooke's Hospital, Cambridge, England.
Lancet Reg Health Eur. 2023 Aug 14;32:100700. doi: 10.1016/j.lanepe.2023.100700. eCollection 2023 Sep.
Methods to identify patients at increased risk of oesophageal cancer are needed to better identify those for targeted screening. We aimed to derive and validate novel risk prediction algorithms (CanPredict) to estimate the 10-year risk of oesophageal cancer and evaluate performance against two other risk prediction models.
Prospective open cohort study using routinely collected data from 1804 QResearch® general practices. We used 1354 practices (12.9 M patients) to develop the algorithm. We validated the algorithm in 450 separate practices from QResearch (4.12 M patients) and 355 Clinical Practice Research Datalink (CPRD) practices (2.53 M patients). The primary outcome was an incident diagnosis of oesophageal cancer found in GP, mortality, hospital, or cancer registry data. Patients were aged 25-84 years and free of oesophageal cancer at baseline. Cox proportional hazards models were used with prediction selection to derive risk equations. Risk factors included age, ethnicity, Townsend deprivation score, body mass index (BMI), smoking, alcohol, family history, relevant co-morbidities and medications. Measures of calibration, discrimination, sensitivity, and specificity were calculated in the validation cohorts.
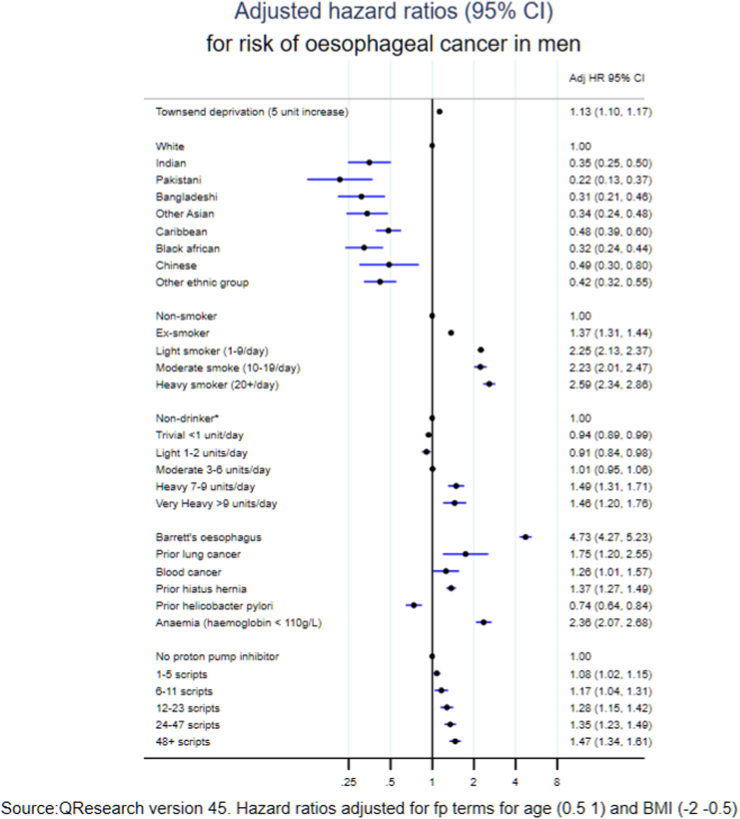
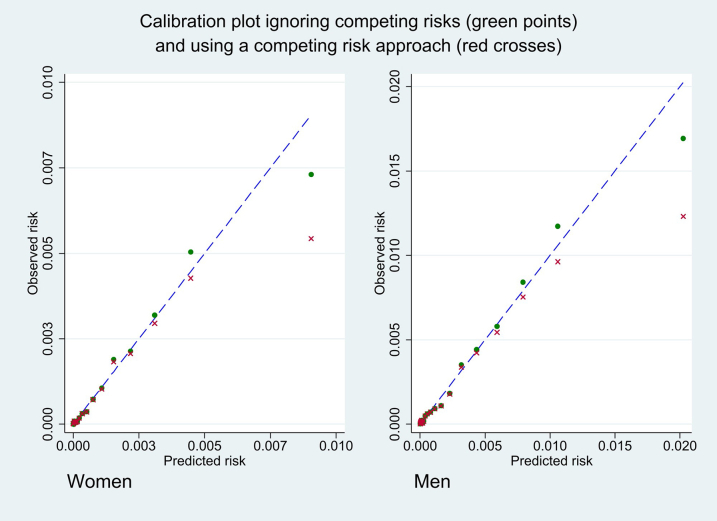
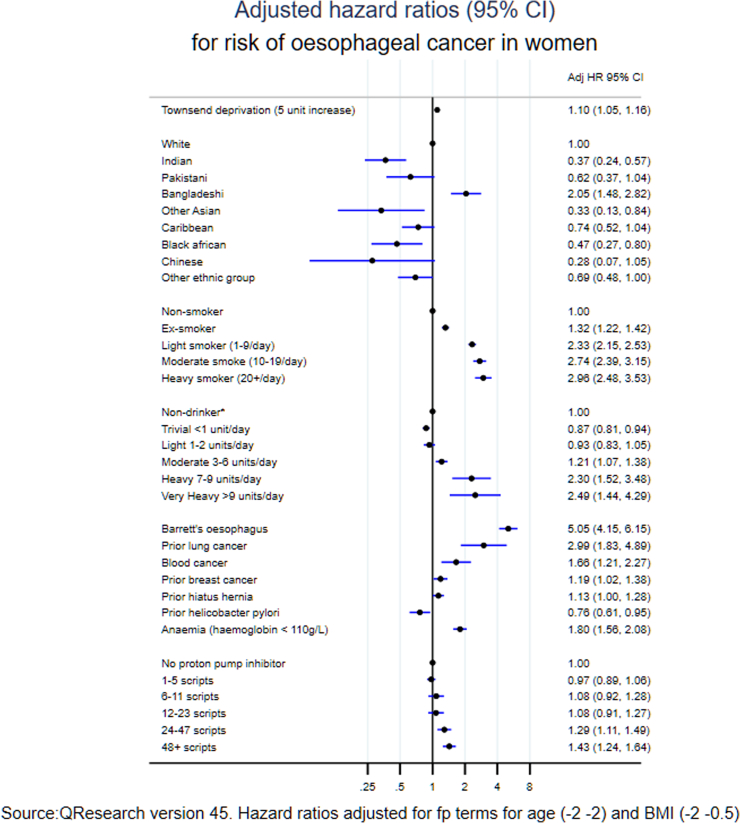
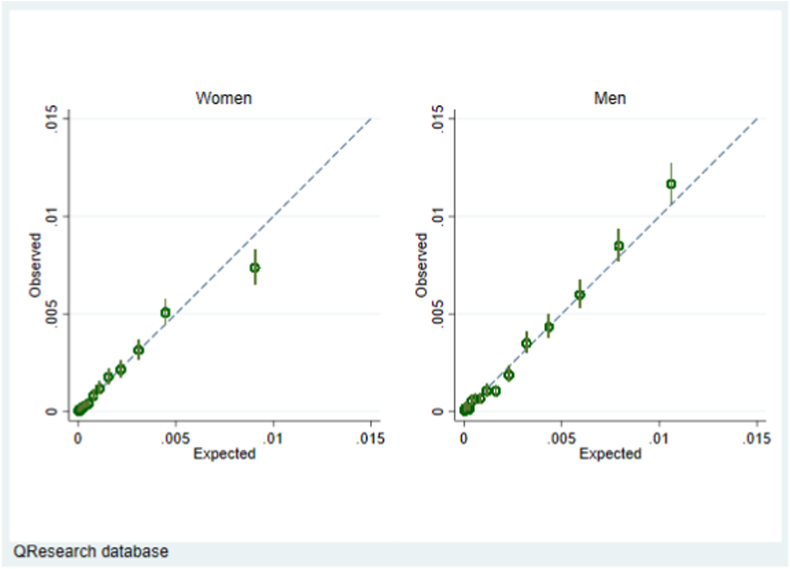
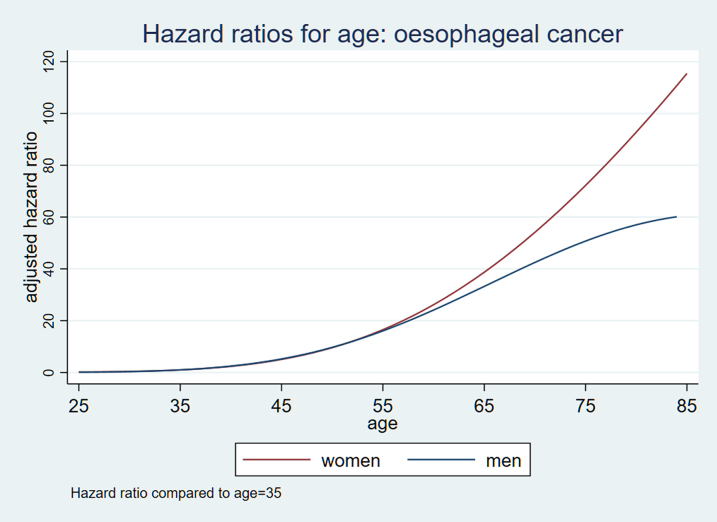
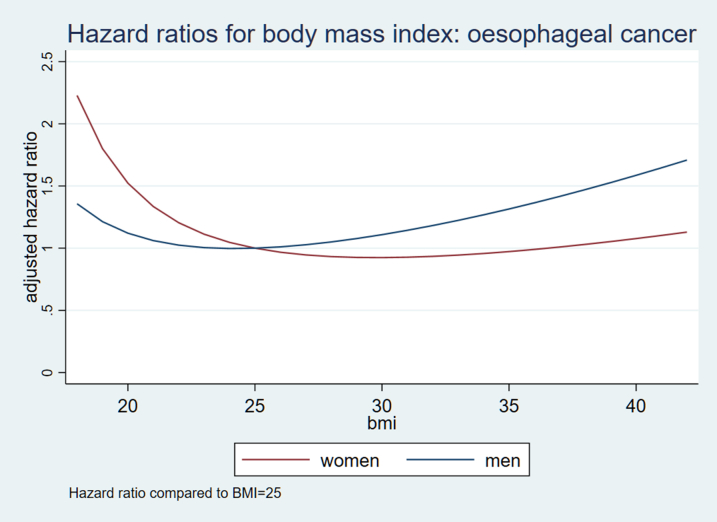
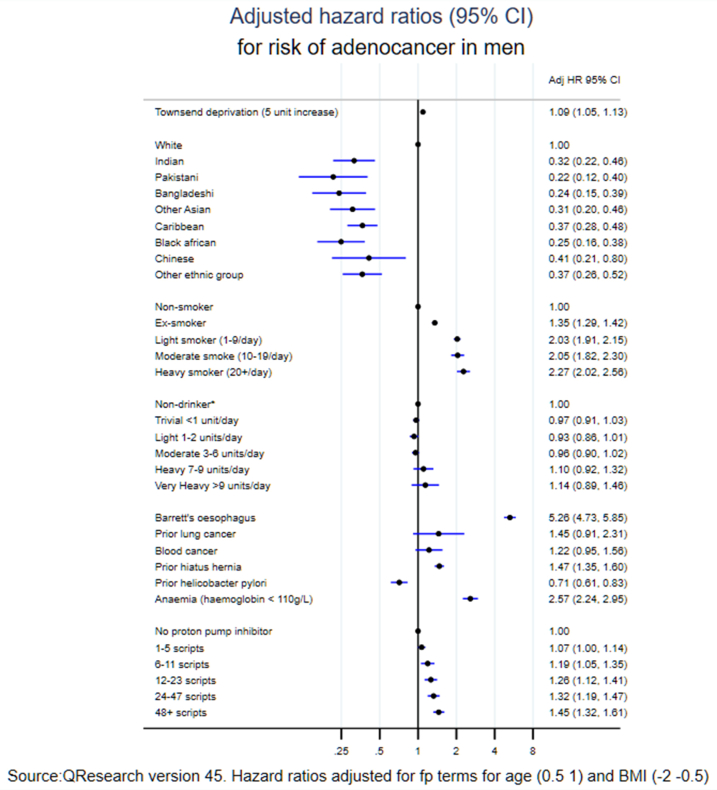
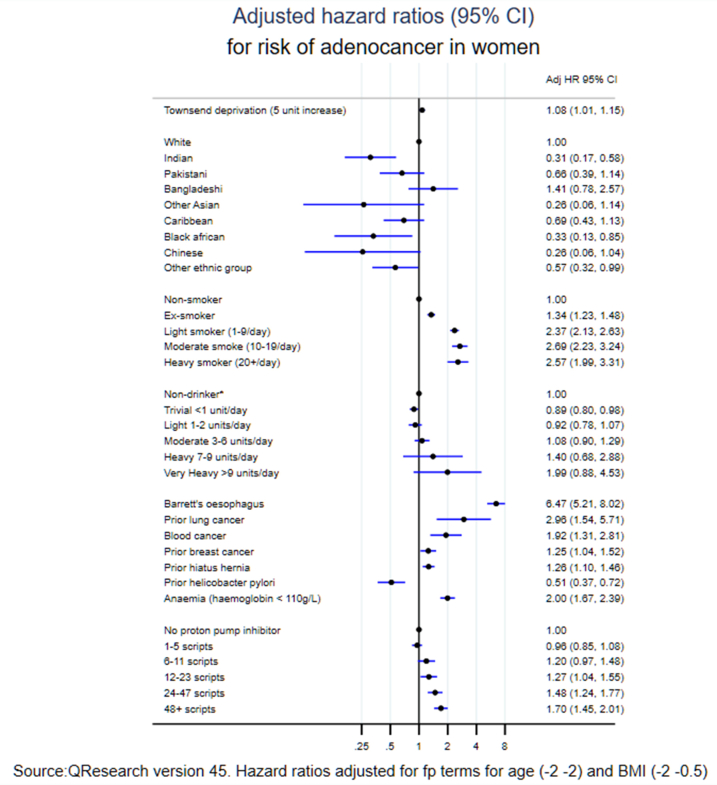
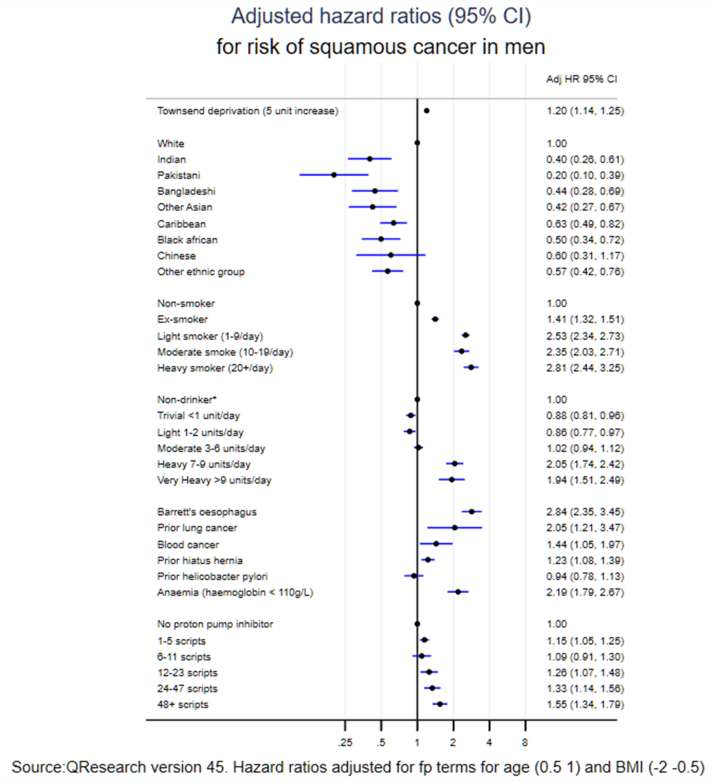
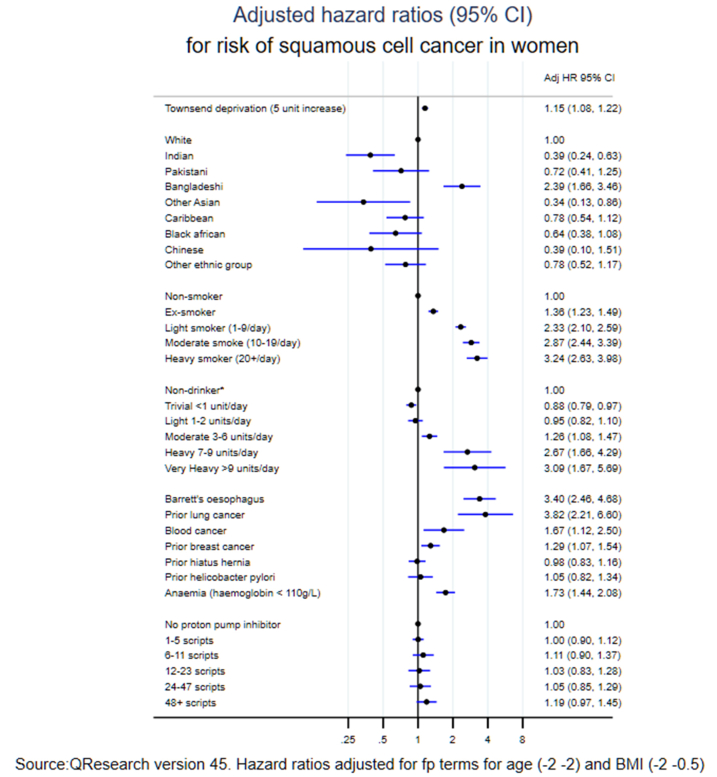
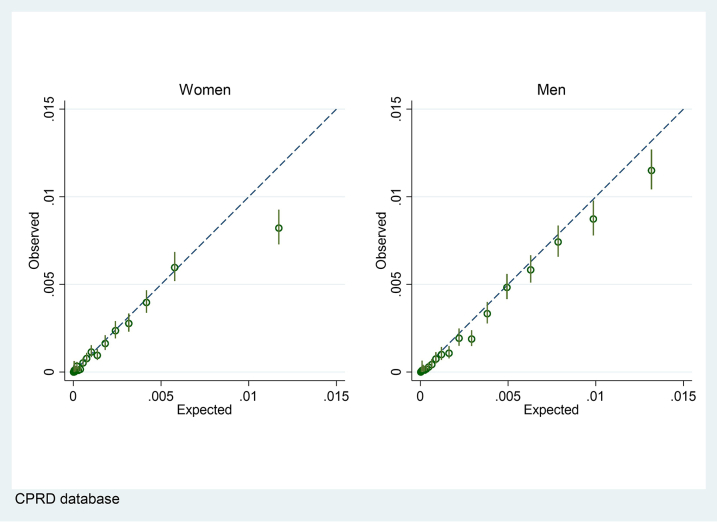
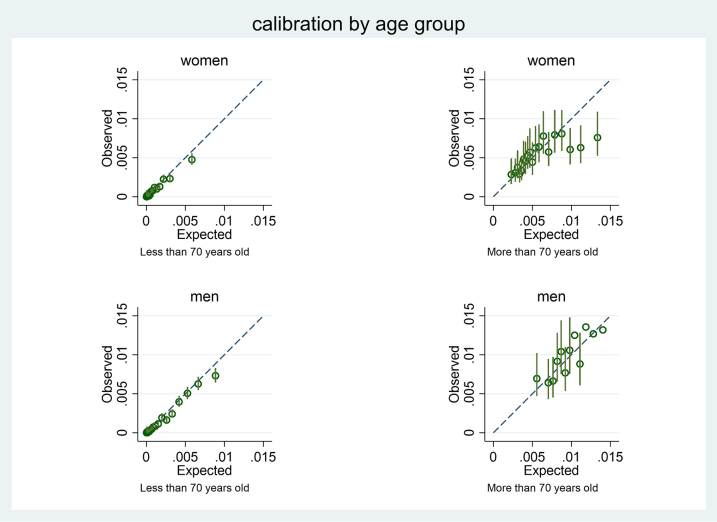
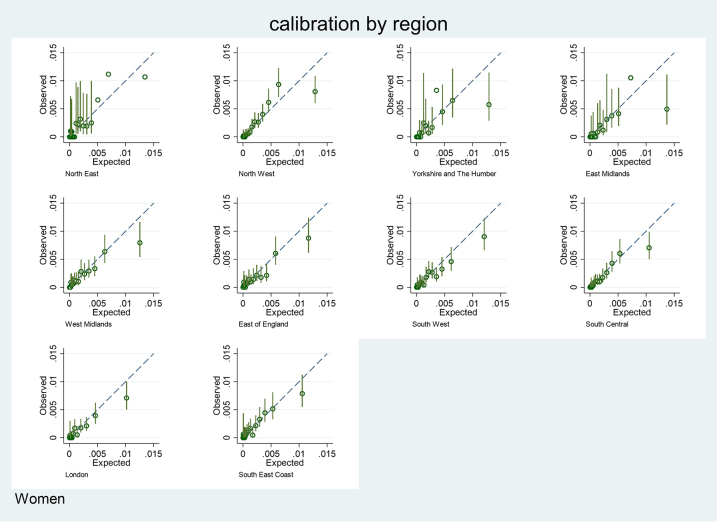
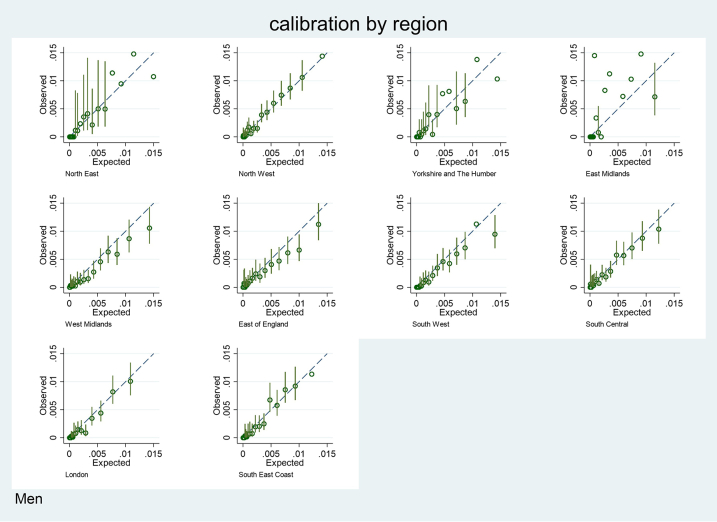
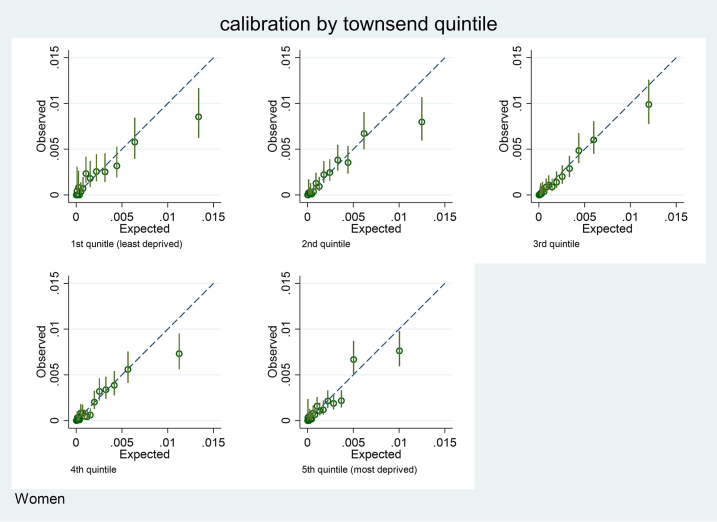
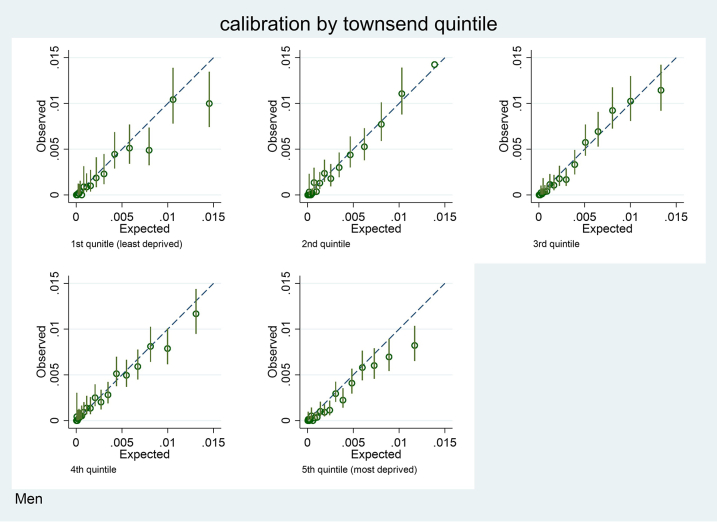
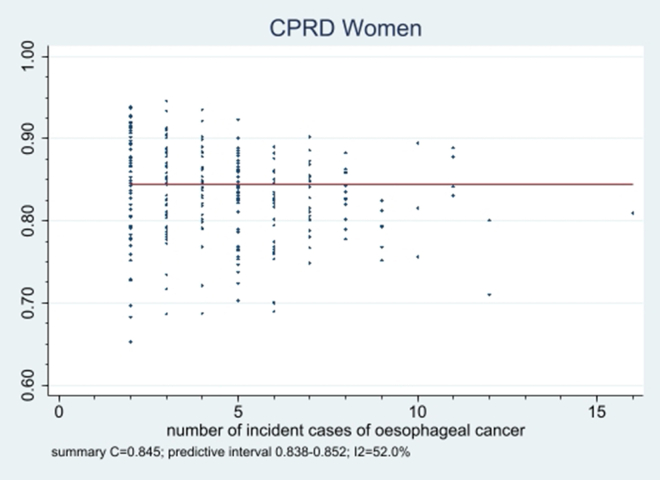
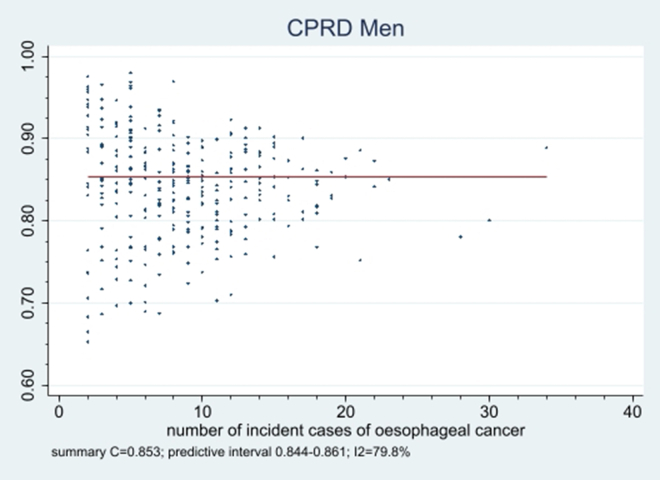
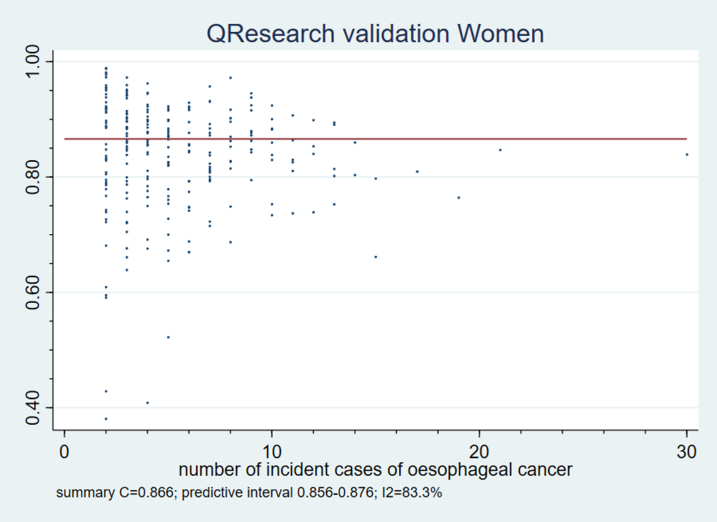
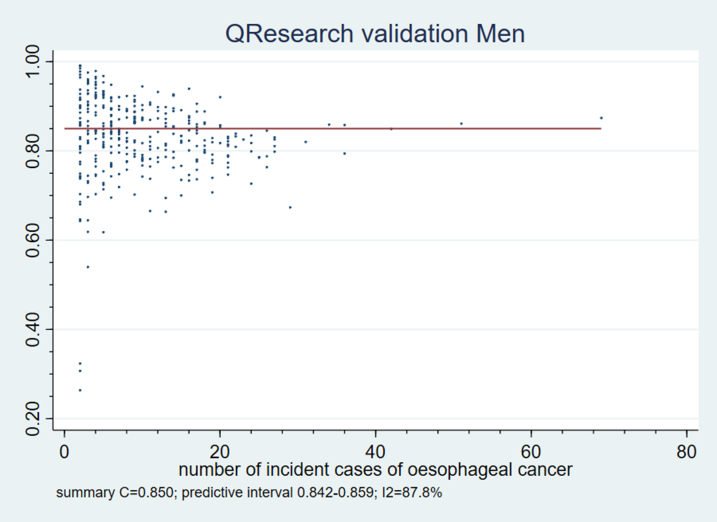
There were 16,384 incident cases of oesophageal cancer in the derivation cohort (0.13% of 12.9 M). The predictors in the final algorithms were: age, BMI, Townsend deprivation score, smoking, alcohol, ethnicity, Barrett's oesophagus, hiatus hernia, infection, use of proton pump inhibitors, anaemia, lung and blood cancer (with breast cancer in women). In the QResearch validation cohort in women the explained variation (R) was 57.1%; Royston's D statistic 2.36 (95% CI 2.26-2.46); C statistic 0.859 (95% CI 0.849-0.868) and calibration was good. Results were similar in men. For the 20% at highest predicted risk, the sensitivity was 76%, specificity was 80.1% and the observed risk at 10 years was 0.76%. The results from the CPRD validation were similar.
We have developed and validated a novel prediction algorithm to quantify the absolute risk of oesophageal cancer. The CanPredict algorithms could be used to identify high risk patients for targeted screening.
Innovate UK and CRUK (grant 105857).
需要有方法来识别食管癌风险增加的患者,以便更好地确定那些适合进行靶向筛查的人群。我们旨在推导并验证新的风险预测算法(CanPredict),以估计食管癌的10年风险,并与其他两种风险预测模型比较性能。
采用前瞻性开放队列研究,使用从1804个QResearch®全科医疗诊所常规收集的数据。我们用1354个诊所(1290万患者)来开发该算法。我们在来自QResearch的450个独立诊所(412万患者)和355个临床实践研究数据链(CPRD)诊所(253万患者)中验证该算法。主要结局是在全科医生、死亡率、医院或癌症登记数据中发现的食管癌确诊病例。患者年龄在25 - 84岁之间,基线时无食管癌。使用Cox比例风险模型和预测选择来推导风险方程。风险因素包括年龄、种族、汤森德剥夺评分、体重指数(BMI)、吸烟、饮酒、家族史、相关合并症和药物。在验证队列中计算校准、区分度、敏感性和特异性的指标。
在推导队列中有16384例食管癌确诊病例(占1290万的0.13%)。最终算法中的预测因素为:年龄、BMI、汤森德剥夺评分、吸烟、饮酒、种族、巴雷特食管、食管裂孔疝、感染、质子泵抑制剂的使用、贫血、肺癌和血癌(女性为乳腺癌)。在QResearch验证队列中,女性的解释变异(R)为57.1%;罗伊斯顿D统计量为2.36(95%置信区间2.26 - 2.46);C统计量为0.859(95%置信区间0.849 - 0.868),校准良好。男性的结果相似。对于预测风险最高的20%人群,敏感性为76%,特异性为80.1%,10年观察到的风险为0.76%。CPRD验证的结果相似。
我们已经开发并验证了一种新的预测算法,以量化食管癌的绝对风险。CanPredict算法可用于识别适合靶向筛查的高危患者。
英国创新署和英国癌症研究中心(资助编号105857)。